

Post-Laminectomy Syndrome (Persistent Spinal Pain)
If you are still in pain after spinal surgery, you are not alone. Studies suggest up to 20–40% of patients experience persistent pain after procedures such as laminectomy, discectomy, or fusion. Instead, they are left asking:
“Why is my pain worse?”
“Did my back surgery fail?”
“Why does my MRI look fine, but I still cannot function?”
Persistent pain after spinal surgery is now clinically termed Persistent Spinal Pain Syndrome Type 2 (PSPS-T2). It affects a significant proportion of patients following lumbar surgery. In many cases, the issue is not surgical failure but scar tissue formation, nerve sensitisation, or ongoing neuroinflammation, all of which require structured specialist assessment.
Post-Laminectomy Syndrome (Persistent Spinal Pain Syndrome Type 2) refers to ongoing back or leg pain that persists beyond the expected healing period after spinal surgery.
Key takeaways
A New Name: “Failed Back Surgery Syndrome” (FBSS) is now clinically referred to as Persistent Spinal Pain Syndrome Type 2 (PSPS-T2).
Not a “Failure”: Persistent pain is often not a result of a surgical error, but a complex response of the nervous system and the development of scar tissue.
The Cause: Primary pain drivers include epidural fibrosis (scar tissue), nerve trauma or injury, nerve sensitisation, and recurrent disc issues.
Advanced Solutions: Modern treatments move beyond medication to include epidural adhesiolysis, pulsed radiofrequency, and neuromodulation techniques like intrathecal pumps and in some instances spinal cord stimulation (SCS).
Multimodal Care: A multimodal approach, combining specialist medical management with interventional procedures, is the gold standard for recovery.
What is it? (Definition)
Post-laminectomy syndrome describes a condition where chronic pain persists or develops following a back or spinal surgery. While the name specifically mentions “laminectomy,” this syndrome can occur after any spinal procedure, like discectomies or fusions stabilisations.
Clinically, it is defined by pain in the back or legs (radicular pain) that does not resolve as expected during the post-operative healing window. It represents a disconnect between a “structurally successful” surgery and the patient’s ongoing physical experience of pain.
Did You Know? (A Shift in Terminology)
For decades, this condition was labelled “Failed Back Surgery Syndrome” (FBSS). This term is increasingly rejected by the global medical community because it implies that the surgeon or the patient “failed”.
In modern pain medicine, we now use the term Persistent Spinal Pain Syndrome Type 2 (PSPS-T2). This shift recognises that the pain is a biological reality caused by neuroinflammation, scar tissue, or a sensitised nervous system and not a failure of character or surgical craft.
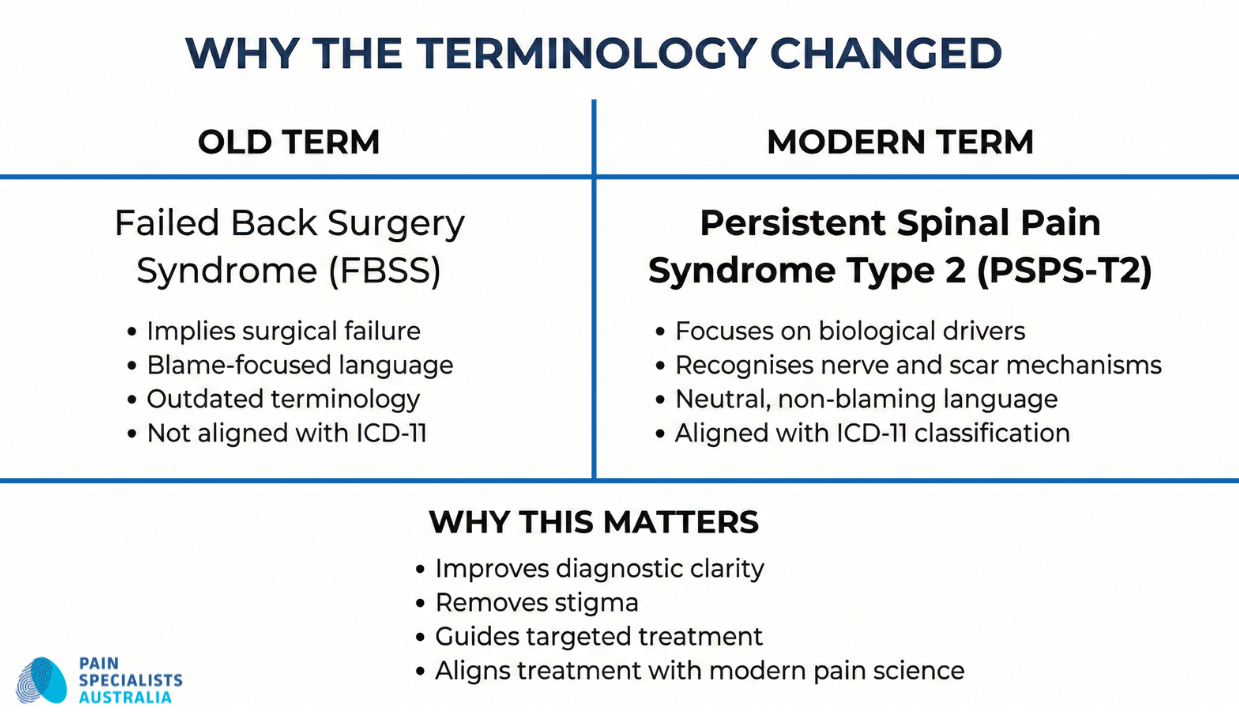
Modern pain medicine now uses Persistent Spinal Pain Syndrome Type 2 instead of Failed Back Surgery Syndrome.
What Does it Feel Like? (Symptoms and Signs)
Common clinical signs of post-laminectomy syndrome include:
Diffuse, dull aching pain in the lower back or surgical site.
Sharp, pricking, or electric-shock sensations radiating into the legs.
Numbness or “pins and needles” in the feet or calves.
Reduced mobility and a feeling of “heaviness” in the lower limbs.
Why Does Pain Persist After Spinal Surgery?
Back surgery can fix structure but still trigger biological changes in the nervous system.
Pain may persist when:
Scar tissue (epidural fibrosis) tethers a nerve root
A previously compressed nerve remains hypersensitive
Adjacent spinal levels develop increased mechanical stress
The spinal cord amplifies pain signals (central sensitisation)
Persistent pain does not automatically mean the surgery failed. It often reflects biological changes in the nervous system.
What Patients Describe: The Lived Experience of Post-Surgical Pain
In clinical practice, imaging findings often represent only part of the overall pain picture. In people experiencing persistent pain after spinal surgery, symptoms may reflect changes in nerve sensitivity rather than a clear structural abnormality on scans.
Patients commonly describe sensations such as:
“It feels like my legs are made of lead.”
“I feel like there is a tight hot band wrapped around my waist.”
“I get sudden ‘zaps’ of electricity that make my leg buckle.”
“It’s like walking on hot coals or broken glass.”
“My surgeon says the MRI looks perfect, but I feel like my back is in a vice.”
If these descriptions sound familiar, you may find our deeper guide on why pain persists after surgery helpful in understanding the transition from acute to chronic pain.
What Causes It? (Pathophysiology)
This video provides general information only and is not a substitute for individual medical advice. Outcomes and treatment suitability vary. Accessing this content does not establish a doctor-patient relationship. Any case studies mentioned are hypothetical.
Understanding why pain persists is the first step toward stopping it. As Dr. Nick Christelis explains in our video, clinical pathophysiology deep-dive, the causes are rarely a single factor; they are usually a combination of biological changes in the nerves and spinal local nerve environment.

Scar tissue after spinal surgery can tether a nerve root and contribute to ongoing pain.
Epidural Post-Operative Fibrosis (Scar Tissue)
Following surgery, the body naturally creates scar tissue as it heals. In some cases, this “fibrosis” becomes excessive. It can bind the delicate nerve roots to the surrounding bone or the surgical site, preventing the nerve from sliding freely. This “tethering” causes significant pain whenever you move.
Nerve Injury And Sensitisation (The “Wind-Up” Phenomenon)
If a nerve was compressed for a long time before surgery, it can remain in a state of “high alert.” This is known as central sensitisation. The spinal cords “volume knob” for pain becomes stuck on high, causing the brain to interpret normal movement or light touch as severe pain.
Recurrent Disc Herniation and Spinal Stenosis
In some instances, the disc at the same level (or the level above) can bulge again, or new bone spurs can create pressure on the spinal canal, leading to recurrent spinal stenosis.
Adhesive Arachnoiditis
This involves inflammation and scarring of the arachnoid membrane (one of the layers protecting the spinal nerves). This causes the nerves to “clump” together, leading to persistent, burning pain and neurological changes which can sometimes even include weakness of the legs.
What Happens Because Of It? (Consequences)
Uncontrolled post-surgical pain often triggers a Downward Pain Spiral.
Ongoing pain often leads to reduced movement, muscle deconditioning, sleep disturbance, and mood changes, which in turn worsen pain perception. This cycle can eventually lead to sleep disturbances, anxiety, depression and a loss of confidence in one’s physical abilities.
How Do You Diagnose It? (Diagnostic Tests)
Before recommending further surgery, we determine whether the pain is structural, inflammatory, neuropathic, or central.
A diagnosis of Post-Laminectomy Syndrome (or now called PSPS-T2) is never made by looking at a scan in isolation. In fact, we often see patients who have been told by their surgical team that the “MRI looks perfect,” yet they remain in devastating pain.
Our diagnostic process used a diagnostic approach. You can watch our video on the ‘Puzzle Piece’ approach to diagnosis to see how we identify the structural and non-structural drivers of your pain.
The Specialist Diagnostic Process
The “Listening Phase”: We don’t just ask where it hurts; we listen to the story of your surgical journey. We identify your unique “Pain Signature”, whether it’s the “heavy lead legs,” the “tight hot bands” around your waist, or the “electric zaps” that cause your leg to buckle. This stage is vital to distinguish between a mechanical structural issue and a sensitised nervous system.
The Structural Screen: While your surgeon has assessed the physical site, we aim to provide an expert, external review of your post-operative scans to rule out the primary structural drivers often seen after laminectomy and would consult with your surgeon if needed. Some questions that may need answering are:
Recurrent Disc Herniation: Has the disc re-prolapsed at the same level or at a new level above or below the surgical site?
Inadequate Decompression: Was the initial pressure on the nerve root or spinal canal fully relieved, or does foraminal stenosis remain?
Spinal Instability: Has the removal of bone during the laminectomy unintentionally affected the stability of that spinal segment?
Advanced Imaging Review: We don’t just read the radiologist’s report; we review the raw data of MRIs and CT scans. We look specifically for the subtle signs sometimes overlooked in general radiology reviews, such as epidural fibrosis (scar tissue), adhesive arachnoiditis, or adjacent segment disease.
Micro-Environment Consideration: Beyond the big structures, we assess inflammatory and neurobiological drivers that may not appear on standard imaging. This includes identifying signs of chemical radiculitis (inflammation that persists even without visible pressure) and the overactive glial cells that keep the pain system switched on long after healing should have occurred long after the tissues have physically healed.
Precision Diagnostic Interventions
Once we have a clinical hypothesis, we use targeted interventions to confirm the source of your pain. If we can “turn off” the pain for even a few hours with a precision block, we have found our answer and the target for your long-term treatment.
Diagnostic Nerve & Joint Blocks: We use local anaesthetic under high-resolution guidance to momentarily quieten specific nerves or the facet joints that may be overcompensating after your surgery.
Epidurography: By using contrast dye under X-ray, we can usually visualise the internal landscape of the spine. This allows us to see exactly where scar tissue (fibrosis) is tethering a nerve root and preventing anti-inflammatory medication from reaching the source of the pain.
How Do You Treat It? (Treatments)
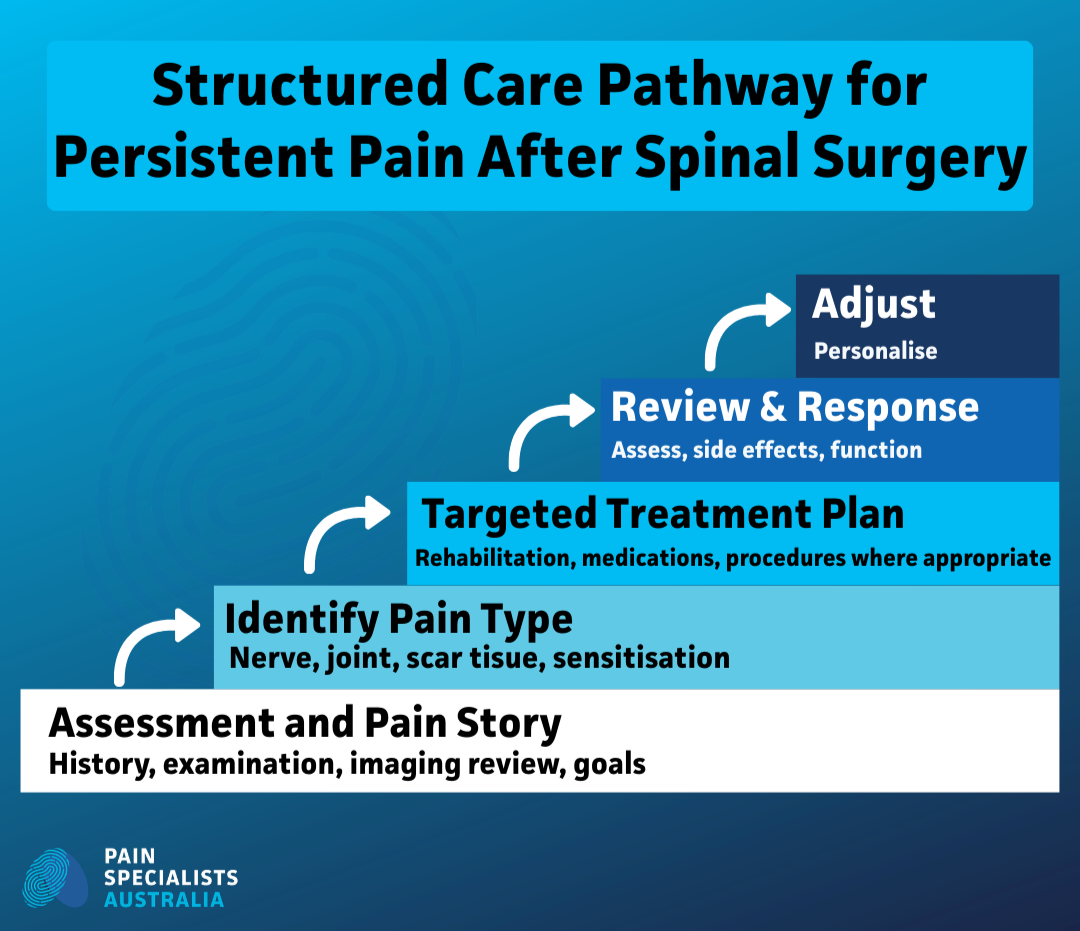
Chronic pain after surgery is managed through structured assessment, targeted treatment, and ongoing review.
Studies show up to 20-40% of patients experience persistent pain after spinal surgery.
At Pain Specialists Australia, we believe there is no one-size-fits-all treatment for chronic pain after spinal surgery. Because the causes of your pain are complex, our response must be equally sophisticated. We utilise a multimodal roadmap that moves beyond simply suppressing symptoms; we treat the entire pain pathway to get you back on track.
Multimodal Medication Management
We don’t just throw medications at the problem. We use a cautious, balanced approach to suppress pain signals and reduce the hyperexcitability of your nervous system. This involves:
Targeted Neuropathic Modifiers: Using anti-convulsants, tricyclics, or SNRIs to “turn down the volume” on hypersensitive nerves.
Specialised Infusions: In specific cases, we utilise ketamine or lidocaine infusions to break the cycle of severe neuropathic pain.
Rationalising Opioids: We help you navigate the pros and cons of opioid therapy, focusing on long-term risks versus short-term gains, tailored specifically to your age and clinical profile.
Nutraceutical Support: Incorporating evidence-based supplements like PEA or Alpha-Lipoic Acid to support nerve health from the inside out.
Epidural Adhesiolysis & Hydrodilation (Breaking Scar Tissue)
Clinical studies (LINK TO Manchikanti et al., 2019) show adhesiolysis is more effective than standard injections for post-surgical scar tissue.
For patients with significant scarring, we perform epidural adhesiolysis. Using a specialised catheter, we gently “wash out” inflammatory proteins and mechanically break down scar tissue (fibrosis) to free the trapped nerve.
Pulsed Radiofrequency (PRF) For Nerve Signal Resetting
For nerves that remain in a state of high alert, we use Pulsed Radiofrequency. This doesn’t burn or damage the nerve; instead, it uses a small electrical field to reset the way the nerve communicates with your brain, providing a targeted signal interrupt to chronic pain.
Advanced Neuromodulation: Spinal Cord Stimulation (SCS)
When pain is refractory in carefully selected cases we may consider Advanced Pain Therapies like Nerve or Spinal Cord Stimulation. By using gentle electrical pulses to mask pain signals before they ever reach the brain, we can provide meaningful pain reduction and improved function in carefully selected patients.
Intrathecal Therapy: Targeted Delivery For Severe Cases
In complex circumstances where oral medications cause too many side effects, Targeted Drug Delivery allows us to deliver medication directly into the spinal fluid. This uses a tiny fraction of the dose required by tablets, focusing the treatment exactly where it is needed most.
Treating The Whole Person
We never treat the pain in a silo; we treat the person. This means managing the physical and the psychological state concurrently:
Movement is Medicine: Overcoming kinesiophobia (fear of movement), using specialised physical therapy to retrain your body to move safely again.
Mindfulness & Stress Reduction: Stress directly impacts pain recovery; we incorporate stress management techniques to help settle your nervous system.
Lifestyle Factors: We look at the low hanging fruit like, diet, smoking cessation, and weight management, that can significantly impact your overall well-being and pain levels.
Why Choose Pain Specialists Australia For Post-Surgical Recovery?
Chronic pain after spinal surgery is complex and requires more than a standard approach. At Pain Specialists Australia, we combine Fellowship-trained expertise with structured, evidence-based care to identify the true pain driver and guide recovery.
Specialist Expertise & Experience
All physicians are Fellowship-trained (FFPMANZCA) pain specialists, and are integrated within major Melbourne private hospitals. Our pain specialists regularly perform adhesiolysis, PRF, and more advanced neuromodulation procedures if needed.
Dual-Qualified Leadership: Our clinic is led by pain specialists with more than 20 years of experience in both anaesthesia and pain medicine, providing a unique perspective on the “micro-environment” of the spine.
Extensive Clinical Experience: Since opening, our team has assessed and treated more than 24,000 people with complex pain conditions across Melbourne.
Specialised in PSPS-T2: We diagnose and treat persistent pain after spine surgery frequently.
Our Puzzle Piece Philosophy
The “Specialist Diagnosis” Approach: We don’t just treat the “spot” that hurts; we piece together the structural and non-structural factors, like glial cell malfunction and neuroinflammation, that keep you in pain.
The “Right” Treatment Framework: We follow a strict protocol to ensure the right patient gets the right treatment for the right reason at the right time.
Beyond the Scan: We recognize that an MRI doesn’t always show the full story. We look for subtle signs of adjacent segment disease or epidural fibrosis that are often overlooked in general reviews.
Advanced Solutions
Minimally Invasive Interventions: From epidural adhesiolysis to pulsed radiofrequency, we offer sophisticated alternatives to “re-operation” that target pain at its source without the trauma of further major surgery.
Neuromodulation: We perform interventional pain procedures within major Melbourne private hospitals, including targeted drug delivery and spinal cord stimulation (SCS), using these tools cautiously to achieve meaningful pain reduction.

Image-guided procedures allow precise treatment of targeted pain sources after spinal surgery.
A Partnership for Recovery
Managing the Person and the Pain: We treat you as a whole being. This means concurrently managing your pain while supporting your physical movement, psychological health, and lifestyle factors.
Empowerment through Education: Our goal is to put you back in the driving seat by helping you understand exactly why you are in pain and providing a clear, evidence-based roadmap for your recovery. We believe that knowledge is power; you can explore our educational video library to learn more about the science of post-surgical pain and the advanced treatments available to you.

Is Revision Surgery Always the Answer?
Revision spinal surgery carries higher risk and often increases scar tissue.
In many cases, the ongoing pain is not due to instability or compression. It is due to nerve tethering, inflammation, or sensitisation.
Identifying this difference is critical before proceeding to another operation.

Frequently Asked Questions (FAQ)
1. Why is my pain worse now than it was before my spinal surgery?
Pain can feel worse after surgery when the procedure fixes the structure but triggers changes in the nervous system. Scar tissue may tether a nerve. The pain system may become over-sensitive. Nearby spinal levels may take extra load and become painful.
Common reasons include:
Epidural fibrosis – scar tissue sticks to a nerve and pulls during movement
Central sensitisation – the nervous system amplifies normal signals into pain
Adjacent segment strain – levels above or below the surgery become stressed
Ongoing nerve irritation – low-grade inflammation around the nerve
Worse pain does not always mean the surgery failed. It often means the pain driver has changed.
2. My surgeon says the MRI looks “normal.” Why am I still in pain?
A normal MRI only shows structure. It does not show how a nerve is functioning. They do not show:
Chemical irritation around a nerve
Small areas of scar tissue tethering
Nerve sensitivity changes
Spinal cord pain amplification
Pain can persist when:
A nerve is chemically irritated without visible compression
Scar tissue limits normal nerve movement
The nerve and spinal cord pain system remains switched on. This is called sensitisation.
Subtle nerve root clumping is missed on routine scans
Pain can be real and severe even when imaging looks stable. Diagnosis requires clinical assessment, not scans alone.
3. Is it too late to get treatment if my surgery was years ago?
No. It is not too late.
The nervous system can change over time. Even long-standing pain can improve with the right approach.
Options may include:
Multimodal rehabilitation to retrain movement and reduce fear
Epidural adhesiolysis for scar-related pain
Pulsed radiofrequency for overactive nerves
Neuromodulation such as intrathecal drug delivery
Chronic does not mean untreatable.
4. Will I need another spinal surgery?
Most people do not need further major surgery. We would work with your surgeon to understand this.
Revision surgery carries higher risk and can create more scar tissue. We focus first on targeted, less invasive options.
These may include:
Image-guided diagnostic blocks
Precision nerve procedures
Neuromodulation instead of structural surgery
The goal is to treat the pain driver without creating more trauma.
5. Can I get back to normal activities?
Many people can return to meaningful activity once the pain driver is identified.
Recovery usually involves:
Reducing fear of movement
Gradually restoring strength and confidence
Combining procedures with rehabilitation
Understanding how your pain system works
The aim is function first. Pain reduction follows.
6. When is pain no longer “normal healing”?
After spinal surgery:
0–6 weeks: Pain and stiffness are expected
3–6 months: Most nerve irritation should settle
Beyond 6 months: Persistent severe pain requires review
Beyond 12 months: Ongoing pain is unlikely to represent normal healing
If pain persists past three to six months, it should be properly assessed.
7. When would revision surgery be appropriate?
Further surgery may be considered if there is:
Progressive neurological deficit
Confirmed recurrent compression
Mechanical instability
We work collaboratively with spine surgeons when structural revision is required.
Clinical Summary for Referrers
Persistent Spinal Pain Syndrome Type 2 (PSPS-T2) represents a heterogeneous group of post-surgical pain states.
Common pain drivers include:
Epidural fibrosis
Central sensitisation
Radicular neuropathic pain
Adjacent segment degeneration
Structured assessment including imaging review, targeted diagnostic blocks, and functional profiling is essential before revision surgery is considered.
References
Further reading and references on pain after spinal surgery:
1. Christelis N, et al. Persistent Spinal Pain Syndrome: A Proposal for Failed Back Surgery Syndrome and ICD-11. Pain Medicine. 2021 Apr 20;22(4):807-818. doi: 10.1093/pm/pnab015.
In this landmark international consensus paper, Pain Specialists Australia founder, Dr. Nick Christelis and a global panel of experts propose replacing the outdated and stigmatised term “Failed Back Surgery Syndrome” (FBSS) with Persistent Spinal Pain Syndrome (PSPS). The paper outlines a new classification system (Type 1 and Type 2) to align with the World Health Organization’s ICD-11. It provides a more accurate medical framework for understanding why pain persists after surgery, focusing on the biological and neurological drivers rather than “surgical failure.”
https://pubmed.ncbi.nlm.nih.gov/33779730/
2. Simpson B, Christelis N, Russo M, Stanton-Hicks M, Barolat G, Thomson S. Will persistent spinal pain syndrome replace failed back surgery syndrome? European Journal of Pain. 2021 Oct;25(9):2076-2077. doi: 10.1002/ejp.1848.
In this expert correspondence, Dr. Nick Christelis and his colleagues address the clinical necessity of transitioning away from “Failed Back Surgery Syndrome” (FBSS). The authors argue that FBSS is a flawed and stigmatising diagnostic label that fails to accurately describe the complex pathophysiology of post-surgical pain. They advocate for the adoption of Persistent Spinal Pain Syndrome (PSPS) as a superior term that is physiologically oriented and avoids the negative connotations of “failure.” The paper reinforces that PSPS provides a clearer framework for medical professionals to discuss causation—whether the pain was caused by surgery, exacerbated by it, or persisted despite it—leading to more targeted and empathetic patient care.
https://pubmed.ncbi.nlm.nih.gov/34339554/
3. Schug SA, et al. The IASP classification of chronic pain for ICD-11: chronic post-surgical or post-traumatic pain. Pain. 2019;160(1):45-52.
This paper outlines the World Health Organisation’s (WHO) updated ICD-11 definitions. It establishes “Chronic Post-Surgical Pain” as a legitimate medical diagnosis, helping patients get recognized by insurers and the broader medical community.
https://pubmed.ncbi.nlm.nih.gov/30586071/
4. Racz GB, Heavner JE, Trescot A. Percutaneous lysis of epidural adhesions—evidence for safety and efficacy. Pain Practice. 2008 Jul-Aug;8(4):277-86. doi: 10.1111/j.1533-2500.2008.00203.x.
This seminal review by the pioneer of the Racz Procedure (Epidural Adhesiolysis) evaluates the clinical safety and effectiveness of using a specialised catheter to physically and chemically break down scar tissue (epidural adhesions). The study provides robust evidence that for patients suffering from post-laminectomy pain, this minimally invasive intervention is superior to standard epidural steroid injections. It highlights how freeing “tethered” nerve roots from fibrosis can significantly reduce pain and improve physical function, establishing the procedure as a primary evidence-based solution for Persistent Spinal Pain Syndrome Type 2.
https://pubmed.ncbi.nlm.nih.gov/18503627/
5. Manchikanti L, Knezevic NN, Sanapati MR, Boswell MV, Kaye AD, Hirsch JA. Effectiveness of Percutaneous Adhesiolysis in Managing Chronic Central Lumbar Spinal Stenosis: A Systematic Review and Meta-Analysis. Pain Physician. 2019 Nov;22(6):E523-E550.
This comprehensive systematic review and meta-analysis evaluates the long-term effectiveness of percutaneous adhesiolysis (the Racz procedure) specifically for patients with chronic central lumbar spinal stenosis. After reviewing multiple randomised controlled trials, the authors concluded that adhesiolysis provides significant, long-term relief from pain and improves functional status for patients who have failed conservative management. The study confirms that by targeting the epidural space to reduce neuroinflammation and mechanical “tethering” of nerves, this intervention offers a high level of evidence-based success for complex spinal pain.
https://pubmed.ncbi.nlm.nih.gov/31775400/
6. Deer TR, Hayek SM, Grider JS, et al. The Polyanalgesic Consensus Conference (PACC)®: Intrathecal Drug Delivery Guidance on Safety and Therapy Optimization When Treating Chronic Noncancer Pain. Neuromodulation. 2024 Oct;27(7):1107-1139. doi: 10.1016/j.neurom.2024.03.003.
This 2024 international consensus document provides the definitive global guidelines for the use of Intrathecal Drug Delivery Systems (IDDS or “pain pumps”). The panel of experts emphasizes that for patients with refractory chronic pain, including those with persistent post-surgical pain, targeted delivery of medication directly into the spinal fluid is a highly effective “therapy optimization” strategy. The guidance focuses on enhancing patient safety and long-term efficacy, noting that this method allows for significantly lower doses of medication compared to oral alternatives, thereby reducing systemic side effects while maximizing pain control in the most complex cases.
https://pubmed.ncbi.nlm.nih.gov/38752946/
7. Jitsinthunun T, Li C, Ng TK, Zinboonyahgoon N. Pulsed Radiofrequency Treatment: Evidence for and Applications in Chronic Pain. Pain Physician. 2025; 28:467-481.
This 2025 narrative review provides a comprehensive update on the clinical evidence and fundamental principles of Pulsed Radiofrequency (PRF) in chronic pain management. The authors highlight PRF as a safe, non-ablative neuromodulatory technique that utilizes high-intensity electrical fields to induce long-term depression of synaptic pain signaling. Crucially for post-surgical patients, the review supports the effectiveness of PRF for radicular pain and persistent spinal pain syndrome (PSPS-T2), particularly when utilizing transforaminal or caudal epidural approaches. The study details how PRF selectively modulates C-fiber nociceptive pathways while promoting long-term nerve regeneration and tissue healing, making it a superior alternative to thermal ablation for mixed somatic nerves.
https://painphysicianjournal.com/current/pdf/ODA2Nw==/173
8. Yoon JP, Son HS, Lee J, Byeon GJ. Multimodal management strategies for chronic pain after spinal surgery: a comprehensive review. Anesthesia and Pain Medicine (Seoul). 2024 Jan;19(1):12-23. doi: 10.17085/apm.23122.
This 2024 comprehensive review provides a modern framework for managing the complex nature of persistent pain after spinal surgery. The authors emphasize that because post-surgical pain involves a mix of structural, neuropathic, and inflammatory drivers, a single-treatment approach is rarely successful. The study advocates for multimodal management, which mirrors the Pain Specialists Australia “Multimodal” roadmap, combining advanced interventional procedures (like SCS and Adhesiolysis) with pharmacological optimisation and psychological support. It highlights the importance of early intervention to prevent the transition from acute post-operative distress to long-term chronic pain.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10847004/
9. Hussain A, Erdek M. Interventional pain management for failed back surgery syndrome. Pain Practice. 2014 Jan;14(1):64-78. doi: 10.1111/papr.12035.
This comprehensive review examines the transition from structural spinal issues to chronic pain states. It argues that “failed back” pain is rarely a result of a single factor but is a complex syndrome involving the epidural space, nerve roots, and facet joints. The authors provide a clinical framework for interventional treatments, emphasizing that once “re-operation” has been ruled out, the focus must shift to managing neuroinflammation and mechanical entrapment (fibrosis). It validates the use of targeted blocks and adhesiolysis as essential tools for identifying and treating the specific “pain generators” that standard imaging often overlooks.
https://pubmed.ncbi.nlm.nih.gov/23374545/
10. Glinka Przybysz A, Vu TN, et al. A systematic review of evidence comparing spinal cord stimulation to sham or conservative medical management in the treatment of persistent spinal pain syndrome - Type 2. Interventional Pain Medicine. 2025 Aug 22;4(3):100635. doi: 10.1016/j.inpm.2025.100635.
This 2025 systematic review is the most current high-level meta-analysis evaluating the efficacy of Spinal Cord Stimulation (SCS) for PSPS-T2 (formerly Failed Back Surgery Syndrome). After a rigorous assessment of the latest clinical trials, the study provides robust evidence that SCS is significantly superior to both sham treatments and conventional medical management in reducing chronic post-surgical pain and improving functional disability. The research underscores that spinal cord stimulation may be considered in carefully selected patients who have not responded to targeted interventional and rehabilitation strategies.
