
Radiofrequency Ablation Explained: RFN vs PRF for Chronic Pain
If medication, injections, or even surgery have not treated your chronic pain, radiofrequency ablation is a group of minimally invasive procedures that work on the nerves carrying your pain signal, rather than the structure on your scan.
There are two distinct types, radiofrequency neurotomy (RFN) and pulsed radiofrequency (PRF). They work in different ways, on different nerves, for different types of pain. Choosing the right one starts with a clear pain diagnosis and cause of pain.

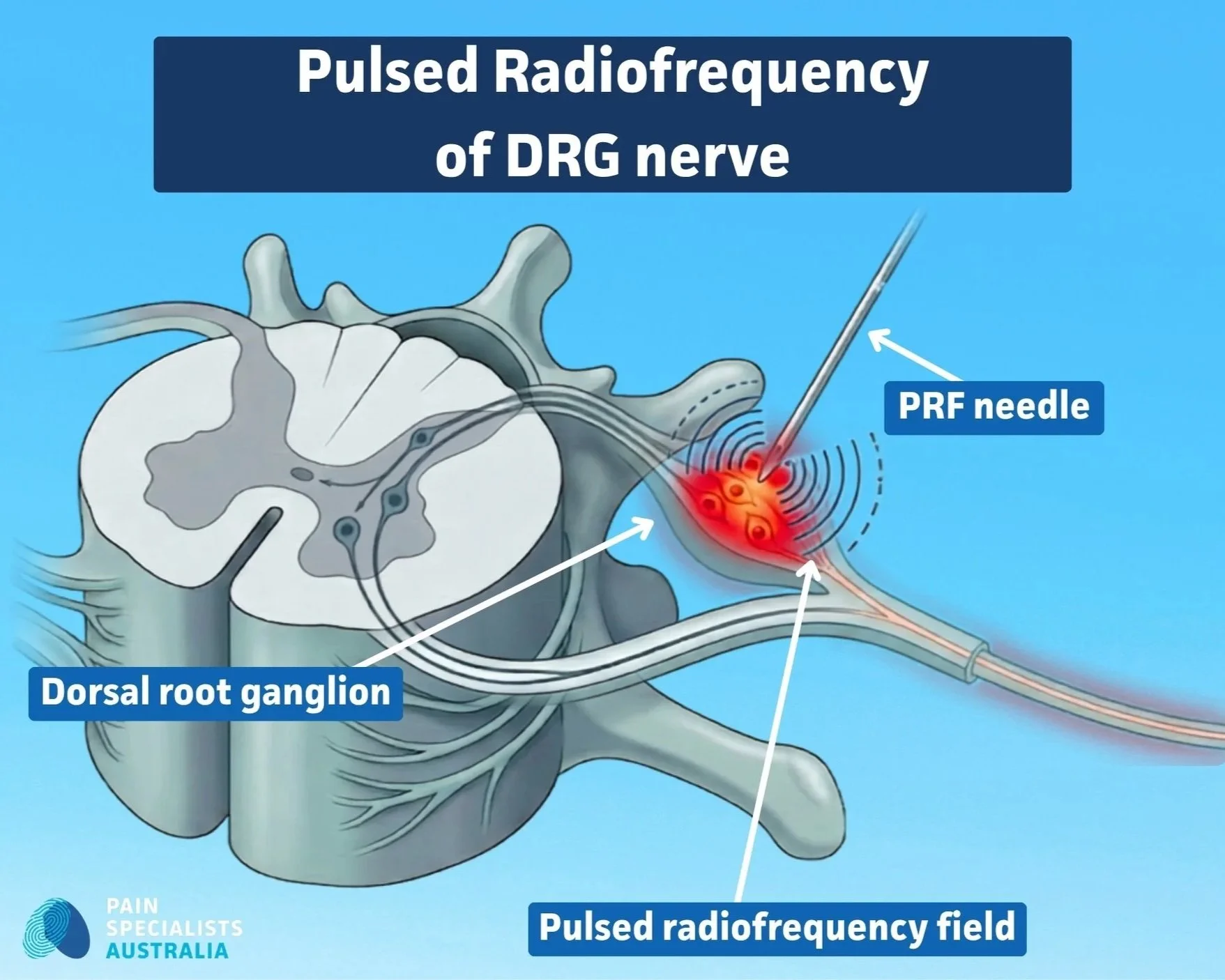
Pulsed radiofrequency of the dorsal root ganglion is performed under fluoroscopic guidance by a specialist pain physician.
What you need to know
Radiofrequency ablation (RFA) works on the nerves (wiring), not the structure (hardware). Radiofrequency ablation targets the nerves sending pain signals, which is why it can help even when scan looks normal.
There are two types of RFA, and the difference matters. RFN uses heat to interrupt pain signals from nerves around a joint. PRF uses gentle electrical pulses to calm an irritated nerve without damaging it.
A test injection usually comes first. A clear, temporary response to a diagnostic block is a good predictor that ablation might help.
Relief is not permanent, but it can be substantial. When it works, most people experience meaningful pain reduction for months, sometimes a year or more, and the procedure can usually be repeated.
It is not only for spine and back pain. RFN and PRF are used across the body, including the neck, face, head, knees, shoulders, hips, and certain types of nerve pain after surgery e.g. persistent spinal pain syndrome (PSPS).
What is radiofrequency ablation, and how does it work?
A trained medical specialist places a thin needle precisely onto a target nerve using imaging guidance (X-ray, ultrasound or CT) and delivers radiofrequency energy through the needle tip to change how that nerve functions. The technique has been used in medicine for decades, including in cardiology and oncology. In pain medicine, the goal is to reduce or interrupt the pain signal from a specific nerve or joint.
How it quietens the nerve sending your pain signal
Pain signals travel along nerves to the brain. When a nerve is overactive, from joint degeneration, nerve injury, or sensitisation, targeting that nerve can reduce or stop the signal getting through. RFN does this with heat. PRF does it with timed pulses that modify how the nerve conducts signals, without temperatures that damage tissue.
What it treats, and what it does not change
Radiofrequency ablation does not fix structural problems. It does not remove arthritis, repair a disc, or reverse nerve damage.
What it can do is interrupt or calm the nerve pathway keeping pain active.
It is most useful when a clear pain generator can be identified and targeted with a needle, and it works best as part of a broader treatment plan.
Burning a nerve versus calming it: RFN vs. PRF
The same machine generates two very different treatments.
Continuous high-temperature energy, interrupting the nerve.
Pulsed low-temperature energy, modifies the nerve function.
Understanding which approach suits your pain is central to getting the right outcome.
Find out what might be driving your pain and whether a radiofrequency procedure is a sensible next step for you.
RFN vs PRF: what is the difference, and which one might suit you?
Two distinct procedures, with different mechanisms, indications, and evidence bases. They are not interchangeable.
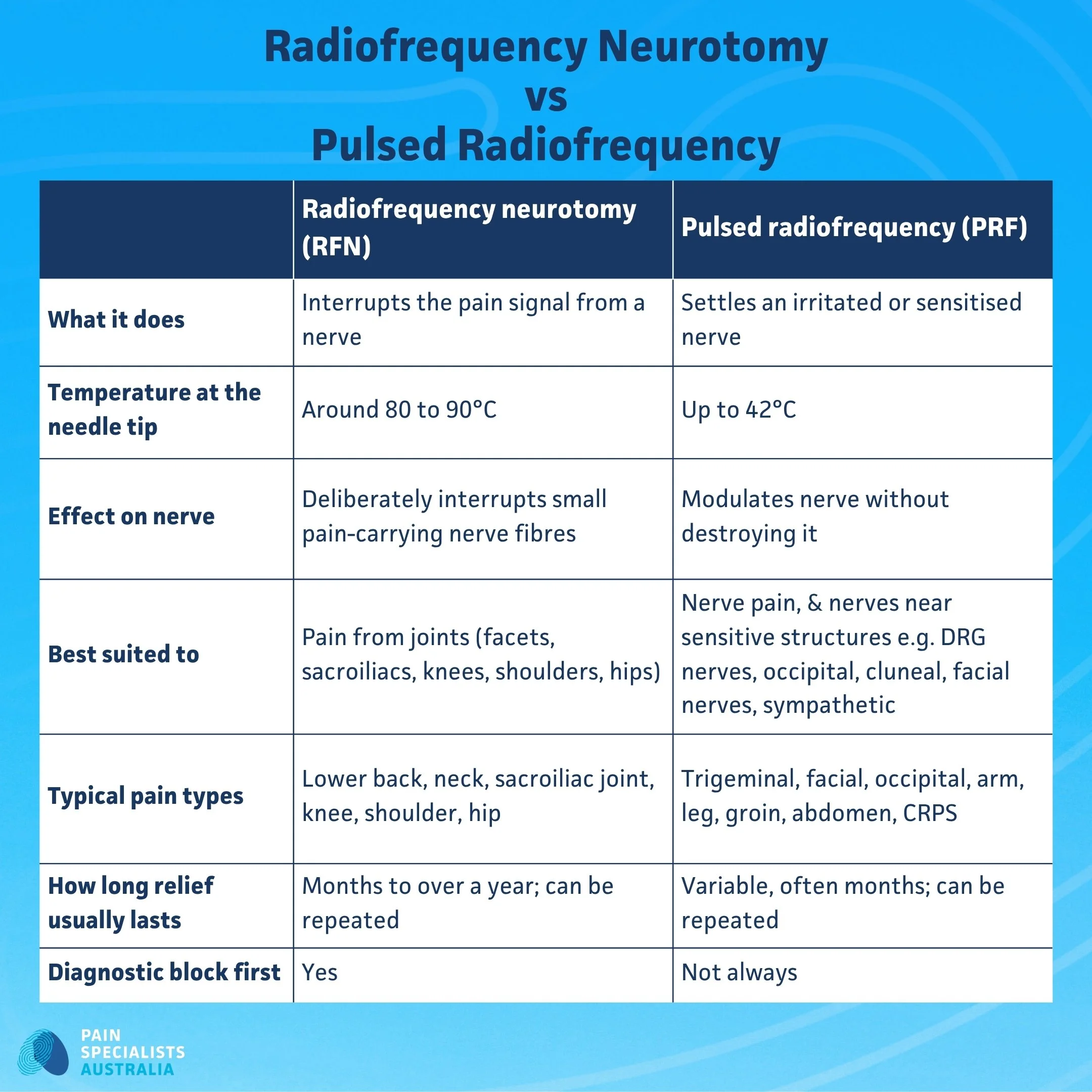
How RFN and PRF differ: temperature, mechanism and the pain they suit.
Radiofrequency Neurotomy (RFN): Interrupting a joint's pain signals

RFN uses heat (80 to 90°C) on small sensory nerves that carry pain from a joint. These nerves do not control movement or limb sensation, so interrupting them does not cause weakness or numbness.
The most common targets are:
Medial branch nerves of the spinal facet joints
Lateral branch nerves of the sacroiliac joint
Genicular nerves of the knee
Articular nerves of the shoulder
Articular nerves of the hip
Selected sympathetic nerve targets for arm pain, leg pain, abdominal and pelvic pain
When the target is right and the technique precise, RFN can provide meaningful relief for six months to two years or more. Because nerves can regenerate, pain can return, and the procedure can usually be repeated. The therapy may not work for some people.
Clinical note: The evidence and research for RFN is strongest for cervical and lumbar facet joint pain and sacroiliac joint pain. Cervical RFN tends to last longer than lumbar, a pattern seen in published studies and clinical experience.
Pulsed Radiofrequency (PRF): Settling an irritated nerve without damaging it
PRF delivers short bursts of radiofrequency energy with the temperature kept below 42°C. The nerve is not destroyed. Instead, the pulses create internal changes that reduce the nerve's ability to transmit pain signals.
Because PRF does not destroy tissue, it suits situations where the target nerve also carries movement or sensation that must be preserved:
Dorsal root ganglion and nerve roots in the neck, chest, back, the dorsal root ganglion, facial nerves
Injured peripheral nerves like the cluneal nerve, brachial plexus, lumbar plexus, and smaller nerves of the arms and legs
PRF typically takes longer to work than RFN. Some people notice improvement within a week or two; others need six to eight weeks or longer, because the effect depends on gradual changes in nerve conduction. The therapy may not work for some people.
Clinical note: PRF is the appropriate choice for neuropathic pain and for nerves where destruction would carry unacceptable risk. The evidence base continues to develop, particularly for radicular pain and dorsal root ganglion applications.
How your pain specialist matches the right technique to the right nerve
The choice between RFN and PRF follows from the diagnosis.
Joint pain from a worn facet or sacroiliac joint points to RFN on the nerve supplying that joint.
Shooting nerve pain down an arm or leg, pain after surgery, or burning pain suggest PRF on the relevant nerve root or ganglion.
Sometimes both are appropriate at different points in treatment.
How do you know if radiofrequency ablation is right for you?
Why a test injection (diagnostic block) usually comes first
Before RFN in particular, your specialist will usually perform a diagnostic block: a small injection of local anaesthetic onto the nerve being considered. It is a test, not a treatment.
If the block gives clear temporary relief (typically 50 to 80% reduction in usual pain for the duration the anaesthetic is expected to work), the nerve is carrying the pain signal. This is one of the strongest predictors of a good response to RFN.
For PRF, a diagnostic block or nerve assessment is often also performed.
What a good response to the block looks like
A positive block means your pain clearly and noticeably reduces for a defined period after the injection.
It does not mean your pain disappears forever; it means the blocked nerve is contributing meaningfully to your pain.
Some specialists perform two separate blocks before proceeding to ablation, because a confirmed positive response improves confidence in the result.
When it may not be the right step for you
Radiofrequency ablation is not for everyone.
It may not be the right next step if a diagnostic block does not provide meaningful relief, if pain is primarily driven by central sensitisation, if the diagnosis is unclear, or if rehabilitation and multidisciplinary care would help more first.
None of this means you are out of options. It means the assessment needs to go further before a procedure is chosen.
See whether a diagnostic block and a structured assessment could give you a clearer picture of your options.
What radiofrequency ablation can treat, from your back to your face
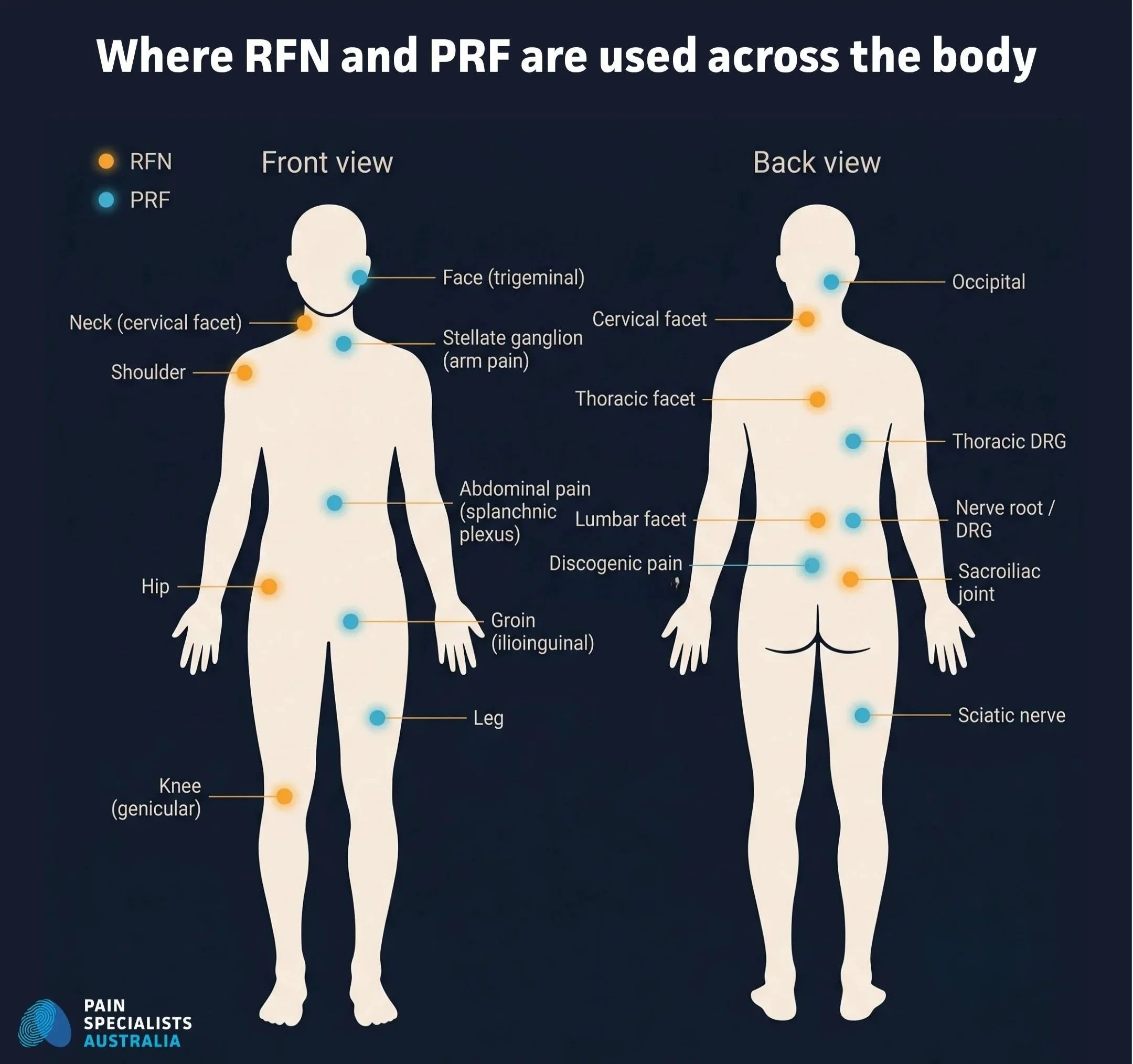
Body map showing where RFN and pulsed radiofrequency are used across the body at Pain Specialists Australia.
Lower back and neck pain from worn joints (facet joint and sacroiliac joint pain)
This is where RFN has its strongest evidence base.
The facet joints are small stabilising joints either side of every spinal vertebra; they wear over time and can drive an aching, stiff back or neck pain that is worse with certain movements.
The sacroiliac joint, where the base of your spine meets your pelvis, can produce low back, buttock or upper-leg pain.
A medial branch or lateral branch block confirms the joint is the source before proceeding to RFN.
When the block is clearly positive and the technique precise, relief can last several months to over a year, and the procedure can be repeated.
A knee that still hurts despite everything (genicular nerve ablation)
The genicular nerves are small sensory nerves carrying pain from the knee joint.
Because they only carry sensation, they can be targeted with RFN without affecting strength or function.
Genicular RFN is used for chronic osteoarthritis knee pain, and for persistent pain after knee replacement when the nerve supply to the joint is contributing. A diagnostic genicular block is performed first.
Stabbing or electric-shock face pain (trigeminal neuralgia and facial pain)
Trigeminal neuralgia produces some of the most intense pain a person can experience, often electric shocks or stabbing triggered by touch, chewing or talking.
When medications are inadequate or their side effects limiting, radiofrequency procedures targeting the trigeminal nerve or its relay point (the Gasserian ganglion) are an established option. Thermal RFN to the Gasserian ganglion has the strongest evidence for longer-term relief in classical trigeminal neuralgia. High voltage PRF to the trigeminal nerve or its branches is also used, particularly when preserving facial sensation is a priority.
The sphenopalatine ganglion (SPG), a nerve bundle deep behind the nose, is another PRF target for selected patients with atypical facial pain or cluster-type headache. Results vary; it is not a first-line standalone treatment.
Headaches at the base of the skull (occipital neuralgia and cervicogenic headache)
Pain at the base of the skull radiating over the back of the head is sometimes driven by the greater and lesser occipital nerves.
When occipital nerve blocks give clear temporary relief, PRF or RFN to these nerves is a considered next step.
Cervicogenic headache, where the upper cervical joints or nerve roots are the source, may be addressed with cervical facet RFN in selected patients.
Still in pain after back surgery (persistent spinal pain syndrome and the dorsal root ganglion)
Persistent pain after spinal surgery (PSPS) is one of the most under-recognised problems in pain medicine.
When surgery is technically successful, but pain continues or changes, the drivers often include nerve sensitisation, scar tissue, ongoing nerve root irritation, or changes at adjacent levels.
The dorsal root ganglion (DRG) sits just outside the spinal cord and acts as a relay point for pain signals. PRF to the DRG is used for persistent radicular pain (leg or arm pain that has not resolved after surgery) when the clinical picture points to ongoing nerve root involvement.
For some patients, PRF is one step in a staged plan that may also include neuromodulation, such as spinal cord stimulation or DRG stimulation.
Ongoing groin pain after a hernia operation (ilioinguinal and genitofemoral nerve pain)
Chronic groin pain after inguinal hernia repair is a recognised complication.
The ilioinguinal, iliohypogastric and genitofemoral nerves can be injured or entrapped during surgery, producing burning, stabbing or aching pain in the groin, inner thigh or scrotum.
When a diagnostic nerve block confirms these nerves are involved, PRF is a considered option, allowing nerve modification without the risks of surgical neurectomy.
It is used within a broader plan that may also include medications, physiotherapy and psychological support.
Stubborn low back and buttock pain that is hard to explain (cluneal nerves and disc-related options)
Not all low back pain and buttock pain comes from facet joints or discs.
The cluneal nerves, small sensory branches over the posterior iliac crest and into the buttock, are an under-recognised source that can mimic facet or sacroiliac pain. PRF or RFN to the cluneal nerves is used for selected patients with a clear, positive diagnostic block.
For carefully selected patients with discogenic low back pain where other structures have been excluded, intradiscal biacuplasty applies bipolar radiofrequency energy inside the back of the disc itself. The evidence base is still developing, and it is considered only within a structured pathway, not as a routine intervention.
Sympathetic nervous system targets (abdominal, pelvic and vascular pain)
Radiofrequency procedures can also target the sympathetic nervous system in selected patients:
Stellate ganglion for facial, ear head and arm pain
Splanchnic plexus or coeliac plexus for abdominal pain
Hypogastric plexus for pelvic pain
Ganglion impar for coccyx and perineal pain
Lumbar sympathetic chain for certain leg or vascular pain conditions
These are specialist procedures used with a clear clinical indication, as part of a broader diagnostic and treatment framework.
CRPS and complex neuropathic pain conditions
Complex Regional Pain Syndrome (CRPS) involves disproportionate, sustained pain with autonomic and inflammatory features that go well beyond the initial injury.
PRF is sometimes used in CRPS as part of a multidisciplinary plan, targeting relevant nerve roots or ganglia in carefully selected patients where a peripheral driver has been identified.
It is not first-line or standalone for CRPS, and is used alongside rehabilitation, medications, psychology, and neuromodulation where appropriate.
CRPS must be treated by specialists in the field of pain medicine.
Anatomy diagram of the spinal facet joint and medial branch nerves targeted in radiofrequency neurotomy.
How long does radiofrequency ablation last?
Realistic expectations by area treated
Duration of relief varies with the nerve targeted, the technique, individual healing, and how well the diagnosis was confirmed. Typical patterns:
Lumbar facet RFN: 6 to 12 months, sometimes longer
Cervical facet RFN: often 12 months or more, sometimes substantially longer
Sacroiliac joint RFN: 6 to 12 months
Genicular nerve RFN: 6 to 12 months in a proportion of patients
PRF to nerve roots and dorsal root ganglion: onset 1 to 8 weeks; duration variable, depending on the underlying condition
PRF for facial pain: outcomes vary with the specific nerve targeted and the underlying diagnosis
These are realistic ranges, not guarantees. Some people experience relief beyond these timeframes; others experience less.
Why pain can come back, and can you have it done again?
For RFN, pain can return because the nerve regenerates. This is expected biology, not a failure.
When pain returns, the procedure can usually be repeated.
Many patients have multiple rounds over years and often find the intervals between treatments gradually extend.
One treatment working doesn’t always mean the next treatment will help.
For PRF, nerve regeneration is less relevant; the question is more often whether the original effect was sufficient and whether the underlying condition has changed.
What to expect on the day, and during recovery
On the day of your procedure
These are day procedures, performed in an accredited facility, with a pre-procedure assessment and time to ask questions.
RFN is typically performed under light sedation with local anaesthetic; some patients choose minimal sedation, others prefer slightly deeper sedation.
PRF can sometimes be performed with local anaesthetic alone. Imaging guidance (usually fluoroscopy or ultrasound) is used throughout.
For RFN, stimulation testing confirms the needle is on the target nerve and away from structures that should not be ablated.
You will need someone to drive you home. Procedures typically take 30 to 90 minutes.
Recovery: What is normal, and what is not
After RFN, it is common to feel sore or more uncomfortable in the first one to two weeks. This is a normal inflammatory response, not a failed procedure.
Benefit usually becomes apparent two to four weeks after treatment, sometimes sooner.
After PRF, the effect builds gradually; most people are advised not to judge the outcome until six to eight weeks.
Ice, anti-inflammatories, and short-term nerve pain medications are commonly used, and your specialist will give you a specific plan.
Possible side effects and risks
All interventional procedures carry some risk, and informed consent involves a thorough discussion with your specialist before you proceed.
For RFN, potential risks include a post-procedure pain flare in the first two to four weeks (common and expected), temporary skin numbness over the treated area, rarely unintended nerve effects if needle position is not adequately confirmed, and uncommon infection, bruising or bleeding at the needle site.
For PRF, the risk profile is generally considered lower because tissue is not destroyed. Main risks are post-procedure soreness, delayed or incomplete response, and rarely local nerve irritation.
Serious complications from either procedure are uncommon, but can occur, even when performed by a trained specialist using imaging and stimulation confirmation.
Clinical note: Stimulation testing before RFN is an important safety and accuracy step. Technique matters significantly to both safety and outcome.
What if you have had radiofrequency ablation and it did not work?
A previous RFA that did not help does not mean the radiofrequency treatment will never work again.
In most cases, there is a reason it did not work, and that reason can often be identified.
Common reasons a procedure does not help
The diagnosis was incomplete or incorrect. If the targeted nerve was not the main pain generator, ablating it will not help. This is why a clearly positive diagnostic block matters.
The technique was not adequately confirmed. Needle placement must be precise, and stimulation testing should confirm proximity to the nerve before energy is delivered.
The wrong type of radiofrequency was used. RFN for neuropathic pain, or PRF for a joint that needed thermal ablation, can both fail for straightforward mechanistic reasons.
A significant central sensitisation component. When the nervous system is broadly sensitised, targeting one peripheral nerve may not be enough on its own.
Unrealistic expectations. RFN and PRF are pain reduction tools, not cures, and work best within a structured plan.
What your next options can look like
A thorough reassessment is the right starting point:
Review the diagnosis
Review what was done and how
Consider whether a different nerve or technique is more appropriate and assess whether a neuromodulation approach might be the better next step
We see many patients who have had procedures elsewhere that did not help. In a significant number of cases, the assessment reveals a modifiable reason, and a different approach produces a better result.
What people describe when they come to us
We listen closely to what people considering radiofrequency ablation share in our Melbourne clinics and in patient online forums and communities. Lived experience helps shape how we assess and support each new patient.
Common patterns include:
Wanting a straight answer on whether it is worth doing, and how long relief might last, before committing to another procedure
Not understanding why a test injection is needed before the main treatment, especially after a long wait
Feeling sore or worse in the first week or two and worrying something has gone wrong, when it is often part of normal recovery
Feeling let down after a previous ablation elsewhere that did not help, and not knowing whether to try again
Being unsure whether RFN, PRF, or neither is the right fit, and wanting it explained properly before deciding
Hoping to reduce their reliance on medication and get back to sleeping, moving and doing the things they value
Why choose Pain Specialists Australia?
Radiofrequency procedures are only as good as the diagnosis and technique behind them. We approach every patient with a diagnosis-first framework. We do not recommend a procedure because it is available; we recommend it because the clinical picture, the diagnostic block, and your goals all point to it as a meaningful step in the process of recovery.
Our specialist pain physicians have extensive experience with RFN and PRF across the full range of applications, from common spinal targets to less frequently treated nerves in the face, groin, and sympathetic system. We use imaging guidance and stimulation testing to confirm needle position before every RFN, and we take time to set realistic expectations.
We also do not dismiss patients who have had procedures elsewhere that did not help; reassessment often reveals a clearer path forward.
Specialist pain physicians with FFPMANZCA fellowship-level training
Diagnosis-led assessment before any procedure is recommended
Imaging-guided technique with stimulation confirmation for RFN
Procedures performed in accredited day procedure facilities
Clinics in Richmond, Heidelberg and Bayside (Sandringham)
Multidisciplinary support including allied health and psychology, when needed
Ask your GP or specialist for a referral to Pain Specialists Australia.
We see patients at our Richmond, Heidelberg, and Bayside clinics.

Frequently Asked Questions (FAQ)
1. How long does radiofrequency ablation actually last?
Spinal facet RFN typically lasts 6 to 18 months, with cervical often longer than lumbar.
Genicular knee RFN can last up to 24 months in some patients.
PRF takes longer to take effect (often 4 to 8 weeks) and has more variable duration. When pain returns, the procedure can usually be repeated.
This treatment doesn’t work for everyone.
2. Does it hurt, and what does it feel like?
Most people have light sedation for RFN with local anaesthetic to the treatment area.
There is usually some discomfort during needle placement and stimulation testing, and it is common to feel sore for one to two weeks afterwards.
PRF is generally associated with less post-procedure soreness.
3. What is the difference between RFN and pulsed radiofrequency (PRF)?
RFN uses heat (80 to 90°C) to interrupt the nerve, suiting joint pain where the target nerve does not carry movement or limb sensation.
PRF uses bursts of energy kept below 42°C to modify the nerve without destroying it, suiting nerve pain, neuropathic conditions, and nerves that carry functions you need to keep.
4. How do I know if I am a candidate?
The most reliable predictor is a positive response to a diagnostic block.
If a small local-anaesthetic injection onto the target nerve gives you clear temporary relief, it is a strong signal that ablating or modifying that nerve is likely to help.
In some cases, diagnostic blocks may not be needed.
5. Is it normal to feel worse in the first couple of weeks?
For RFN, yes. The heat causes a local inflammatory reaction that can temporarily increase pain before it improves. It is not a sign of failure. Ice, anti-inflammatories, and short-term nerve medications help.
For PRF, a mild flare is also possible, and benefit may not be apparent for four to eight weeks.
6. Do the nerves grow back, and can I have it done again?
After RFN, the treated nerve can regenerate, which is why pain can return. This is expected biology.
When it does, the treatment can usually be repeated, and some patients find successive treatments produce progressively longer intervals of relief.
With PRF, regeneration is less relevant because the nerve was not destroyed.
7. Why might radiofrequency ablation not work?
Common reasons include an incomplete diagnosis, imprecise needle placement, the wrong type of radiofrequency for the pain, or a significant central sensitisation component.
A reassessment often clarifies what went wrong and whether a different approach is worth considering.
8. Is radiofrequency ablation covered by Medicare in Australia?
Medicare rebates may apply to procedures performed by qualified specialist physicians in accredited facilities, depending on the procedure and indication.
Out-of-pocket costs vary; confirm with our rooms and your private health insurer.
9. Can I drive or go back to work afterwards?
You cannot drive home after the procedure because of the sedation. Most people rest for the remainder of the day. Light sedentary work is often manageable within a day or two; physical work may require a longer break. Discuss with your specialist beforehand.
10. Can it help nerve pain that has not gone away since my operation?
Yes, this is one area where PRF can be useful.
Persistent nerve pain after spinal surgery, knee replacement, or hernia repair sometimes reflects ongoing nerve irritation that can be targeted.
A careful assessment to confirm which nerve is involved, followed by a diagnostic block, is the right first step.
If the block provides clear temporary relief, PRF or another nerve-directed approach is worth considering within a broader plan.
References
1. Dreyfuss P, Halbrook B, Pauza K, Joshi A, McLarty J, Bogduk N. Efficacy and validity of radiofrequency neurotomy for chronic lumbar zygapophysial joint pain. Spine (Phila Pa 1976). 2000;25(10):1270–7.
This prospective audit established that lumbar medial branch RFN, performed under strict diagnostic and technical conditions, produced clinically meaningful pain relief and improved function, defining the modern standard for patient selection and technique.
https://pubmed.ncbi.nlm.nih.gov/10806505/
2. McDonald GJ, Lord SM, Bogduk N. Long-term follow-up of patients treated with cervical radiofrequency neurotomy for chronic neck pain. Neurosurgery. 1999;45(1):61–7.
A long-term follow-up demonstrating that cervical RFN provides meaningful pain relief that can be reinstated by repeat treatment when the effect wears off, and establishing durability well beyond a year in a significant proportion of patients.
https://pubmed.ncbi.nlm.nih.gov/10414567/
3. Husted DS, Orton D, Schofferman J, Kine G. Effectiveness of repeated radiofrequency neurotomy for cervical facet joint pain. J Spinal Disord Tech. 2008;21(6):406–8.
A retrospective study showing that repeat cervical RFN reproduces the benefit of the initial procedure with similar success rates and duration of relief, supporting the case that the procedure can safely and effectively be repeated when pain returns.
https://pubmed.ncbi.nlm.nih.gov/18679094/
4. Van Boxem K, de Meij N, Kessels A, Van Kleef M, Van Zundert J. Pulsed radiofrequency for chronic intractable lumbosacral radicular pain: a six-month cohort study. Pain Med. 2015;16(6):1155–62.
A six-month cohort study of PRF adjacent to the lumbar DRG in patients with chronic intractable radicular pain, showing meaningful pain reduction and improved function in a substantial proportion, supporting PRF as a considered option for selected nerve root pain.
https://pubmed.ncbi.nlm.nih.gov/25580669/
5. Byrd D, Mackey S. Pulsed radiofrequency for chronic pain. Curr Pain Headache Rep. 2008;12(1):37–41.
A widely cited review explaining that PRF delivers radiofrequency energy without significant thermal nerve damage, and summarising its role, proposed mechanisms and clinical applications across chronic pain conditions.
https://pubmed.ncbi.nlm.nih.gov/18417022/
6. Van Boxem K, van Bilsen J, de Meij N, Herrler A, Kessels F, Van Zundert J, van Kleef M. Pulsed radiofrequency treatment adjacent to the lumbar dorsal root ganglion for the management of lumbosacral radicular syndrome: a clinical audit. Pain Med. 2011;12(9):1322–30.
A large clinical audit of PRF applied adjacent to the lumbar DRG in lumbosacral radicular syndrome, showing meaningful proportions of patients achieving worthwhile pain relief and supporting the role of PRF at the DRG in appropriately selected patients.
https://pubmed.ncbi.nlm.nih.gov/21812907/
7. Van Zundert J, Patijn J, Kessels A, Lamé I, van Suijlekom H, van Kleef M. Pulsed radiofrequency adjacent to the cervical dorsal root ganglion in chronic cervical radicular pain: a double blind sham controlled randomized clinical trial. Pain. 2007;127(1-2):173–82.
The first high-quality trial of pulsed radiofrequency (PRF) applied at the nerve relay point in the neck (the cervical dorsal root ganglion) for stubborn arm pain caused by an irritated nerve root. Patients treated with PRF had significantly better pain relief than those given a placebo procedure, supporting PRF as a considered option for carefully selected patients with cervical radicular pain.
https://pubmed.ncbi.nlm.nih.gov/17055165/
8. Kapural L, Mekhail N. Novel intradiscal biacuplasty (IDB) for the treatment of lumbar discogenic pain. Pain Pract. 2007;7(2):130–4.
The first published description of intradiscal biacuplasty using radiofrequency inside the disc, introducing a minimally invasive option for carefully selected patients with discogenic low back pain refractory to conservative care.
https://pubmed.ncbi.nlm.nih.gov/17559482/
9. Choi WJ, Hwang SJ, Song JG, Leem JG, Kang YU, Park PH, Shin JW. Radiofrequency treatment relieves chronic knee osteoarthritis pain: a double-blind randomized controlled trial. Pain. 2011;152(3):481–7.
This double-blind randomised controlled trial in elderly patients with severe knee osteoarthritis, all selected via a positive diagnostic genicular block, showed that RF neurotomy of the genicular nerves produced significantly greater pain reduction and functional improvement than sham at 12 weeks, establishing genicular RFN as a considered option for carefully selected chronic knee pain.
https://pubmed.ncbi.nlm.nih.gov/21055873/
10. Wan C, Dong DS, Song T. High-voltage, long-duration pulsed radiofrequency on Gasserian ganglion improves acute/subacute zoster-related trigeminal neuralgia: a randomized, double-blinded, controlled trial. Pain Physician. 2019;22(4):361–8.
This randomised double-blinded trial showed that high-voltage, long-duration PRF applied to the Gasserian ganglion was more effective than standard PRF for zoster-related trigeminal neuralgia, supporting the role of optimised PRF parameters when preserving facial sensation matters and thermal RFN is not preferred.
