

Knee Pain That Won’t Go Away: Diagnosis and Treatment in Melbourne
Key Takeaways
Knee pain that does not improve is often not just a joint problem
A normal scan does not rule out real pain - the cause is often in how pain is being generated, not what the scan shows
Nerve-related pain and sensitisation are common and often missed
Persistent pain after injury or surgery usually requires a different approach
Treatment works best when the true cause of pain is clearly diagnosed
Nerve pain and sensitisation after surgery are common, treatable, and frequently missed by standard pathways.
When Knee Pain Doesn’t Improve, Something Is Being Missed
Knee pain that doesn’t improve needs a different approach.
Many people are told their scan is normal, their surgery was successful, or that they just need more time. Yet the pain continues. It may worsen with walking, disturb sleep, or feel out of proportion to what has been found.
In these situations, the issue is often not the joint itself. It is how pain is being generated and processed. Persistent knee pain is frequently driven by nerve sensitivity, inflammation that has not settled, or a diagnosis that has not yet been fully defined.
This is where a specialist assessment changes direction.
Instead of repeating the same treatments, the focus shifts to identifying the true source of pain and building a targeted plan based on that diagnosis. For many people, this is the point where things finally start to make sense.
Why Knee Pain Doesn’t Go Away – the Causes Most People Miss

Comparison of a healthy joint and an osteoarthritic knee with cartilage damage and a rheumatoid arthritis joint with inflammation
Knee pain is often explained as a simple joint problem.
In reality, persistent knee pain is usually more complex. Many people are treated for the obvious cause, but the real driver of pain is either incomplete, misunderstood, or missed entirely.
Understanding these different pain mechanisms is the first step toward getting the right diagnosis.
Joint Related Knee Pain
Osteoarthritis (wear and tear)
Rheumatoid arthritis
Gout and pseudogout
Septic arthritis (infection)
If your pain feels worse than what your scan shows, the joint may not be the full explanation.
Nerve-Related Knee Pain - When the Problem Is the Wiring, Not the Joint
Not all knee pain comes from the joint. In many cases of persistent knee pain, the joint is not the main problem at all. The problem is the nervous system.
Understanding this distinction is one of the most important steps toward getting the right diagnosis.
Most knee pain starts as what clinicians call nociceptive pain. This is the body's normal response to tissue damage, the joint is inflamed, the cartilage is worn, the ligament is torn, and the pain signal reflects that damage accurately. This type of pain generally improves as the tissue heals or the inflammation settles.
Neuropathic pain works differently. Here, the pain is being generated or amplified by the nervous system itself, not by ongoing tissue damage. The nerves around the knee, or the pathways that carry pain signals from the knee to the brain, become sensitised. They fire more easily, more intensely, and sometimes without any clear trigger.
This is why two people can have the same MRI findings and experience completely different levels of pain. The scan shows the joint. It does not show the nervous system.
Neuropathic or nerve-driven knee pain has a recognisable pattern. If your pain fits this description, it is a significant clinical signal:
Burning, searing, or electric-shock sensation around or below the knee
Pain that is worse at rest or at night, rather than only with movement
Sensitivity to light touch, clothing, bedsheets, or gentle pressure causes pain
Pins and needles, numbness, or a crawling sensation around the knee
Pain that feels disproportionate to what any scan has shown
Pain that spreads beyond the original area or changes location
Sometimes, it’s referred from the spine, hips, or nerves, leading to pain that feels deep, radiating, or out of proportion to local findings.
These features suggest the pain system itself has become overactive. The knee may be the location of the pain, but the driver is neurological.
The hardware and the wiring
A useful way to understand persistent knee pain is to separate two distinct systems.
The hardware is the physical structure of the knee — the bones, cartilage, ligaments, tendons, and the implant if you have had a replacement. This is what scans show. This is what surgery fixes.
The wiring is the nervous system — the network of nerve fibres around the knee, the spinal cord pathways, and the brain's pain processing systems. Scans do not show this. Surgery does not automatically reset it.
When someone is told their X-ray looks perfect after a knee replacement, or that their MRI shows only mild changes, they are being told the hardware is intact or minimally damaged. That is often true. But it tells us nothing about the wiring.
Persistent knee pain, especially pain that is burning, sensitive, or worse at night — is frequently a wiring problem. The structure has been assessed. The nervous system has not.
Why surgery does not always resolve the pain
This is one of the most important and least-explained facts in persistent knee pain.
A technically successful knee replacement or arthroscopy corrects the structural problem it was designed to correct. The implant may be perfectly positioned. The repair may be sound. The surgeon did exactly what was planned.
But surgery does not reset the pain system.
If the nervous system was already sensitised before the operation - which is common in people who have lived with significant knee pain for months or years, that sensitisation does not simply resolve when the joint is repaired. The nerves around the knee may have been irritated or partially injured during the procedure itself. Scar tissue can entrap nerve branches. The central pain pathways can remain in a heightened state even after the peripheral problem has been addressed.
This is why a significant proportion of people who have had technically successful knee surgery continue to experience pain, sometimes pain that is worse than before. It is not a failure of the surgery. It is a failure to address what the surgery was never designed to fix.
Research shows that up to one in five patients experience persistent pain after total knee replacement. In many of these cases, neuropathic mechanisms are a key driver. These patients need a different assessment, not more of the same treatment.
Which Nerves Around the Knee Cause Pain?
Several specific nerve pathways around the knee are known to contribute to persistent pain when irritated or damaged:
Infrapatellar branch of the saphenous nerve — inner and front knee pain, often burning or sharp. Frequently injured during knee surgery and slow to settle.
This video is provided for educational purposes only. It is a clinical discussion by a specialist pain medicine physician and does not constitute specific medical advice. Individual outcomes vary significantly. All treatments and procedures discussed carry risks. Please discuss whether any treatment is appropriate for your specific situation with your treating specialist.
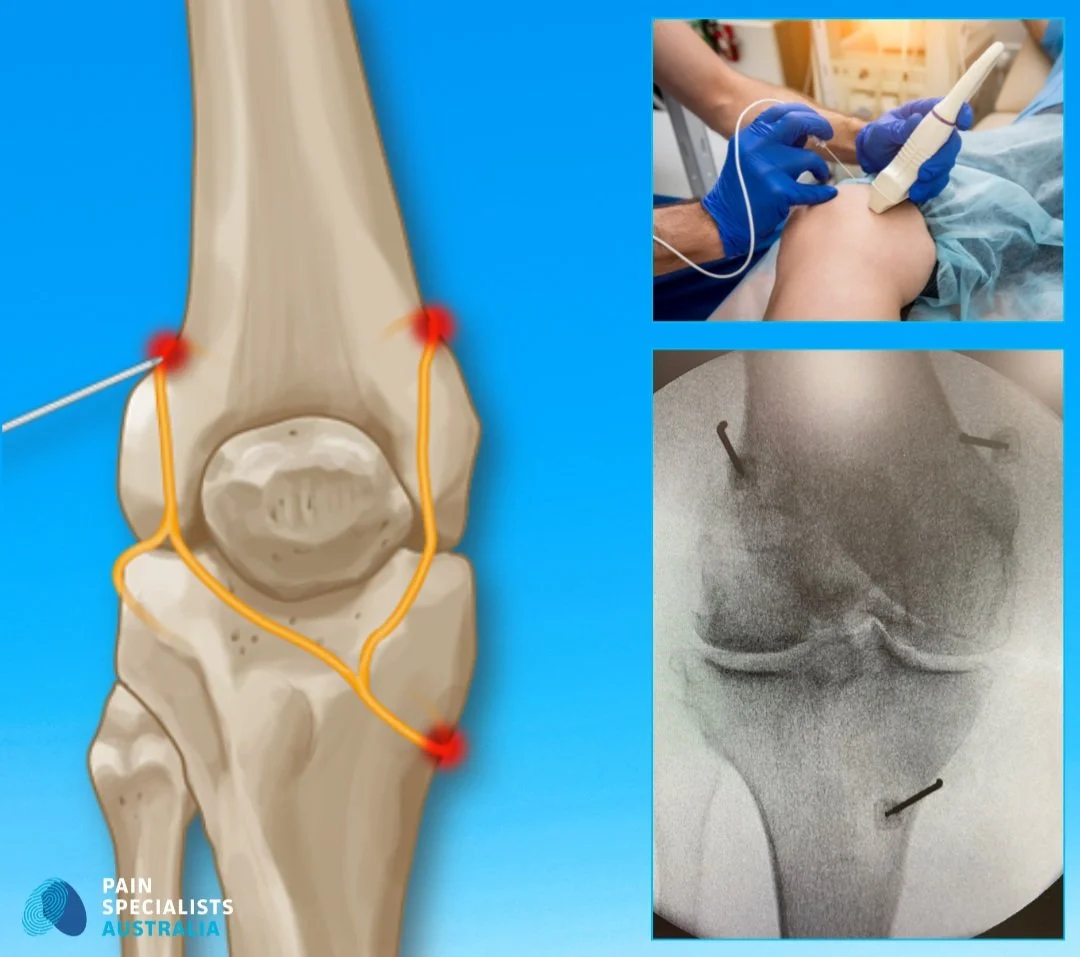
Genicular nerves — small branches that carry pain signals from the joint itself. The target of genicular nerve blocks and radiofrequency ablation.
Common peroneal nerve — outer knee pain, sometimes with numbness or weakness in the lower leg.
Lumbar nerve roots (L3/L4) — referred pain from the lower spine that feels like it is coming from the knee. One of the most commonly missed causes.
Identifying which nerves are involved is not something a scan can do. It requires a structured clinical assessment and, in many cases, targeted diagnostic nerve blocks, where temporarily numbing a specific nerve tells us whether that nerve is contributing to the pain.
This is where a specialist assessment changes what is possible.
Who Is likely to Develop Persistent Knee Pain
Knee pain can affect anyone, but some people are more likely to develop pain that does not settle or becomes chronic.
You may be at higher risk if you:
Are over 40 and starting to notice ongoing knee discomfort
Play high-impact sports or have a history of knee injury
Have had previous knee surgery, including arthroscopy or replacement
Spend long periods sitting or have reduced physical activity
Have a physically demanding job involving lifting, kneeling, or repetitive movement
These factors explain how pain starts, but they rarely explain why it won't stop. When symptoms persist despite treatment, the underlying mechanism is usually more complex than the original trigger.
What People with Persistent Knee Pain Often Describe
People living with persistent knee pain often describe a consistent pattern of experience. Common themes include: pain that continues despite a 'normal' scan result; burning, electrical, or night-time pain that feels disproportionate to imaging findings; multiple treatments tried without lasting improvement; and a sense that the diagnosis has never been fully explained. These experiences are well-recognised in the clinical literature and often signal that the underlying mechanism has not yet been fully identified.
Common experiences include:
“I’ve been told everything looks normal, but the pain is still there”
“I’ve tried physio, injections, even surgery, and nothing has worked”
“The pain is worse at night or feels like burning or sensitivity”
“It doesn’t make sense. The scan doesn’t match how it feels”
“I feel like I’m going in circles without clear answers”
“I've had three cortisone injections. Each one helped for a few weeks, then the pain came straight back.”
These experiences reflect a common problem. The pain diagnosis is often incomplete, and the real driver of pain has not yet been identified.
This is where a structured, specialist assessment can help bring clarity and direction.
What Persistent Knee Pain Actually Feels Like?
Knee pain does not present the same way for everyone. The pattern of symptoms often gives clues about what is driving the pain.

Common Knee Pain Symptoms Include
Deep aching or sharp pain in or around the knee
Stiffness, especially after rest or in the morning
Swelling or a feeling of pressure in the joint
Pain or inability to kneel, or worsening pain when kneeling or crouching
Clicking, grinding, or reduced movement
Weakness or the knee feeling unstable
Redness, warmth, or fever (if infection is present)
Symptoms the Pain may be Nerve-Related
These symptoms are explained in more detail in the nerve pain section above,
When Knee Pain Is Not Improving As Expected
Most knee injuries improve within weeks. When pain continues beyond this, it often means the underlying cause has not been fully identified.
You should consider a pain specialist assessment if:
Your pain has lasted longer than three months
The pain is worsening or not responding to treatment
You are waking at night because of pain
The knee feels unstable or unreliable
The pain feels burning, spreading, or electrical
Your scan looks “normal” but the pain is not
At this stage, repeating the same treatments rarely helps. A different approach is required.
If you have already had surgery, and the surgeon says the joint is fine, and are still struggling with pain, the nervous system might be at fault. Watch Dr. Nick Christelis explain the biology of post-surgical pain i.e. chronic pain after knee replacement.
This video is provided for educational purposes only. It is a clinical discussion by a specialist pain medicine physician and does not constitute specific medical advice. Individual outcomes vary significantly. All treatments and procedures discussed carry risks. Please discuss whether any treatment is appropriate for your specific situation with your treating specialist.
How Knee Pain is Diagnosed
Accurate diagnosis is the most important step in treating persistent knee pain. This requires more than imaging alone.
Before you can treat the symptoms, we must identify the biological cause. As Dr. Nick explains, there is no such thing as generic 'knee pain', it is a symptom of a specific issue like
This video is provided for educational purposes only. It is a clinical discussion by a specialist pain medicine physician and does not constitute specific medical advice. Individual outcomes vary significantly. All treatments and procedures discussed carry risks. Please discuss whether any treatment is appropriate for your specific situation with your treating specialist.
When nerve involvement is suspected, targeted diagnostic nerve injections (nerve blocks) can help confirm the source of pain.
Numbing a specific nerve temporarily, and observing whether the pain improves, gives more useful information than another scan. This is one of the most important diagnostic tools in complex or persistent knee pain, and one that most standard pathways never reach.
A specialist assessment includes:
Clinical assessment
Detailed history of how the pain started and changed
Physical examination of movement, strength, and stability
Assessment of nerve sensitivity and referred pain
Imaging (when needed)
X-ray for joint changes
MRI or CT for soft tissue and structural detail
Ultrasound for dynamic assessment
Scans are helpful, but they do not always explain pain. Many people have abnormal scans with no pain, and others have severe pain with minimal findings.
This is why diagnosis must focus on both structure and pain behaviour.
Treatments Depends on the Correct Diagnosis of Knee Pain
Our clinic uses advanced non-surgical pathways for knee arthritis and osteoarthritis treatment in Melbourne to reduce inflammation and delay the need for joint replacement surgery.
Treatment fails when the diagnosis is unclear. Once the source of pain is identified, treatment becomes targeted and more effective.
Chronic or Persistent Knee Pain
Structured rehabilitation
Pain education and pacing
Targeted medical treatment
Radiofrequency ablation for knee arthritis pain relief
Interventional Pain Procedures
Interventional procedures can play a key part of managing persistent knee pain, especially when medications or physiotherapy alone haven’t worked. These targeted treatments, such as image-guided injections, nerve blocks, and radiofrequency ablation, can provide clinically meaningful and, in some patients, sustained relief by targeting specific pain generators.
Steroid
Genicular nerve blocks
Pulsed radiofrequency (PRF)
Advanced Therapies
For complex or treatment-resistant knee pain, advanced therapies like neuromodulation may be recommended. When structural issues are suspected or ongoing, surgical intervention may be recommended. We collaborate closely with some of Melbourne’s experienced orthopaedic surgeons to ensure coordinated, multidisciplinary care when structural intervention is required.
Neuromodulation
Multidisciplinary care
Referral for orthopaedic surgery if structural damage is present
Any invasive or interventional procedure carries risks. Before proceeding with any treatment, you should discuss the potential risks, benefits, and alternatives fully with your treating specialist. You may also wish to seek a second opinion from an appropriately qualified health practitioner. For persistent knee pain that has not responded to conservative treatment, interventional procedures, including image-guided injections, nerve blocks, and radiofrequency ablation, can offer targeted relief in appropriately selected patients. Results vary. Your specialist will assess whether these approaches are suitable for your specific diagnosis.
LEARN MORE ABOUT OUR TREATMENTS
How to Get Knee Pain Relief in Melbourne
Getting relief from knee pain depends on identifying the real cause, not just managing symptoms. For many people, the standard pathway does not go far enough, especially when pain is ongoing or not improving.
Most people start with their GP. This is an important first step to rule out serious conditions and begin early treatment. However, if your pain continues, the next step is not more of the same. It is a more detailed assessment.
You should consider a specialist pathway if your knee pain:
Has lasted longer than expected
Is not improving with physiotherapy or medication
Feels out of proportion to scan findings
Is affecting your sleep, movement, or daily life
At this stage, a pain specialist can:
Identify whether the pain is joint, nerve, or mixed in origin
Coordinate care with physiotherapy and rehabilitation
Offer targeted treatments such as injections or nerve-based therapies
Build a structured plan based on your diagnosis
This approach shifts the focus from trial-and-error treatment to a diagnosis-led pathway.
For a deep dive into the 'Plumbing vs. Wiring' of the knee, watch our full clinical discussion on diagnosing complex knee pain after knee replacement. A discussion between Dr. Nick Christelis and Dr. Andy Kwok.
This video is provided for educational purposes only. It is a clinical discussion by specialist pain medicine physicians and does not constitute specific medical advice. Individual outcomes vary significantly. All treatments and procedures discussed carry risks. Please discuss whether any treatment is appropriate for your specific situation with your treating specialist.
Fast-track to the insights you need:
[09:16] Plumbing vs. Wiring: Why a surgeon can fix the "plumbing" (the joint), but the "wiring" (the nerves) can still cause pain.
[13:27] Pre-Op Risk Factors: Learn which biological and lifestyle factors increase risk of developing chronic pain after surgery.
[32:29] The Spine Connection: How lower back can mimic "bone-on-bone" knee pain, leading to unnecessary surgeries.
[35:12] Genicular Nerve RFA: A non-surgical option to manage pain.
Frequently Asked Questions (FAQ)

1. What’s the most common cause of knee pain in adults?
The most common cause is osteoarthritis, but it is not the only reason knee pain persists.
Many people have ongoing knee pain due to a mix of joint changes, previous injury, and nerve-related pain. Importantly, scans do not always match symptoms. Some people have severe arthritis with little pain, while others have significant pain with minimal findings.
2. How do I know if my knee pain is serious?
Knee pain is more likely to need specialist assessment if it is not improving or affecting your daily life.
Warning signs include:
Pain lasting longer than a few weeks
Swelling, warmth, or reduced movement
Instability or the knee giving way
Night pain or worsening symptoms
These features may suggest a more complex problem such as joint damage, nerve involvement, or infection.
3. Can chronic knee pain be treated without surgery?
Yes. Most chronic knee pain can be managed without surgery when the correct diagnosis is made.
Treatment options may include:
Physiotherapy and structured rehabilitation
Radiofrequency ablation
Neuromodulation in selected cases
Surgery is usually reserved for clear structural problems that have not responded to other treatments.
4. Do I need a referral to see a knee pain specialist in Melbourne?
Yes. A referral from your GP is required to see a pain specialist and access Medicare rebates.
Your GP also helps rule out urgent conditions and ensures your care is coordinated. If your pain is ongoing or not improving, a referral is the next step.
5. What if I’ve had surgery but still have pain?
Persistent pain after knee surgery is not uncommon and does not always mean the surgery has failed.
In many cases, pain is driven by:
Nerve irritation or injury
Ongoing inflammation
Scar-related changes
Altered pain signalling
A specialist assessment can help identify the cause and guide targeted treatment.
6. Is it normal to have knee pain years after an injury or surgery?
No. While it is common, it is not normal to have ongoing knee pain years later.
Persistent pain often reflects an unresolved diagnosis, nerve sensitisation, or a problem that has not been fully addressed. This is where a structured assessment can make a difference.
7. Why does my knee still hurt when scans are normal?
Knee pain can persist even when scans look normal because not all pain comes from visible structural damage.
Pain may be driven by:
Nerve sensitivity
Referred pain from the spine or hip
Early-stage joint changes not easily seen on imaging
This is a common reason people feel stuck. The scan is not wrong, but it does not explain the full picture.
8. What is the difference between joint pain and nerve pain in the knee?
Joint pain usually feels deep and aching, often worse with weight-bearing and better with rest. Nerve pain tends to feel burning, sharp, or electric, often worse at night and sensitive to touch rather than movement. The distinction matters because these two types of pain respond to different treatments. A specialist assessment can identify which pattern is driving your symptoms, or whether both are present.
READY FOR RELIEF?
When to Seek Urgent Medical Care for Knee Pain
Most knee pain is not dangerous, but some symptoms require urgent assessment.
Seek immediate medical attention if you have:
Sudden, severe pain after an injury or fall
Inability to walk, stand, or put weight on the leg
A visibly deformed knee or suspected fracture
Rapid swelling with severe pain
Fever, chills, or a hot, red, swollen knee
Pain following recent surgery that is getting worse
These symptoms may indicate a serious problem such as fracture, infection, or acute joint injury that requires urgent treatment.
References
If you’re interested in more, here are some references for your perusal.
1. Lankhorst NE, Bierma-Zeinstra SM, van Middelkoop M. Risk factors for patellofemoral pain syndrome: a systematic review. J Orthop Sports Phys Ther. 2012 Feb;42(2):81-94.
- This systematic review identifies overuse, biomechanical factors, and muscle imbalances as key risk factors for developing patellofemoral pain syndrome, especially in active populations.
https://pubmed.ncbi.nlm.nih.gov/22031622/
2. Hunter DJ, March L, Chew M. Osteoarthritis in 2020 and beyond: a Lancet Commission. Lancet. 2020 Nov 28;396(10264):1711-1712.
- This Lancet Commission highlights the growing global burden of osteoarthritis and calls for a shift toward prevention, personalised care, and non-surgical treatment options.
https://pubmed.ncbi.nlm.nih.gov/33159851/
3. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618-25.
- This landmark paper outlines how persistent post-surgical pain affects up to 25% of patients and identifies nerve damage and poor pain control as major risk factors.
https://pubmed.ncbi.nlm.nih.gov/16698416/
4. Duong V, Oo WM, Ding C, Culvenor AG, Hunter DJ. Evaluation and Treatment of Knee Pain: A Review. JAMA. 2023 Oct 24;330(16):1568-1580. doi: 10.1001/jama.2023.19675. PMID: 37874571.
- This JAMA review provides an updated overview of knee pain diagnosis, evaluation and treatment.
https://pubmed.ncbi.nlm.nih.gov/37874571/
5. Mo L, Jiang B, Mei T, Zhou D. Exercise Therapy for Knee Osteoarthritis: A Systematic Review and Network Meta-analysis. Orthop J Sports Med. 2023 Jun 5;11(5):23259671231172773.
- This review found that all exercise types improved symptoms in knee osteoarthritis, with aquatic exercise most effective for pain relief and yoga best for joint stiffness, function, and quality of life.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10280533/
6. Culvenor AG, Øiestad BE, Hart HF, Stefanik JJ, Guermazi A, Crossley KM. Prevalence of knee osteoarthritis features on magnetic resonance imaging in asymptomatic uninjured adults: a systematic review and meta-analysis. Br J Sports Med. 2019 Oct;53(20):1268-1278.
- This systematic review found that MRI features of knee osteoarthritis are common even in asymptomatic, uninjured adults - appearing in up to 43% of those over 40 - highlighting the need to interpret imaging results alongside clinical symptoms.
https://pubmed.ncbi.nlm.nih.gov/29886437/
7. Ohashi Y, Uchida K, Fukushima K, Inoue G, Takaso M. Mechanisms of Peripheral and Central Sensitization in Osteoarthritis Pain. Cureus. 2023 Feb 22;15(2):e35331.
- This review outlines how peripheral and central sensitisation - driven by inflammatory cytokines, nerve growth factor, and serotonin - contribute to osteoarthritis pain, often independent of structural changes, highlighting emerging therapeutic targets.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9949992/
8. Bennell KL, Bayram C, Harrison C, Brand C, Buchbinder R, Haas R, Hinman RS. Trends in management of hip and knee osteoarthritis in general practice in Australia over an 11-year window: a nationwide cross-sectional survey. Lancet Reg Health West Pac. 2021 Jun 9;12:100187.
- Bennell et al. (2021) found that despite rising GP encounters for hip and knee OA in Australia, first-line lifestyle treatments remain underused, with ongoing reliance on imaging and medications.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8356093/
9. Li CY, Ng Cheong Chung KJ, Ali OME, Chung NDH, Li CH. Literature review of the causes of pain following total knee replacement surgery: prosthesis, inflammation and arthrofibrosis. EFORT Open Rev. 2020 Sep 30;5(9):534-543.
Adverse knee pain occurs in 10–34% of all total knee replacements (TKR), and 20% of TKR patients experience more pain post-operatively than pre-operatively.
