

Knee Arthritis Treatment in Melbourne
Key takeaways
Most knee arthritis can be treated without surgery using injections, nerve treatments, and structured rehabilitation.
Night pain, pain with stairs and first steps after sitting are common problems knee arthritis pain we treat.
A clear plan starts on day one with exercise and pain medications.
Injections can help short term; if relief is brief, we plan the next step.
Genicular nerve blocks and ablation can help selected patients.
Knee surgery is considered only when non-surgical treatment fails to control pain or restore function and when daily life stays limited after full care.
What is Knee Arthritis and Why can Pain Spike?
Knee osteoarthritis happens when joint structures change and get irritated. Pain often flares at night, on stairs, and in the first steps after sitting. Swelling can come and go. Scans do not always match how much it hurts. Many people say, “my scan looks mild but my pain is severe.” That mismatch is common. We start with a plan that blends exercise, education, weight support and pacing, then build up treatment as needed.
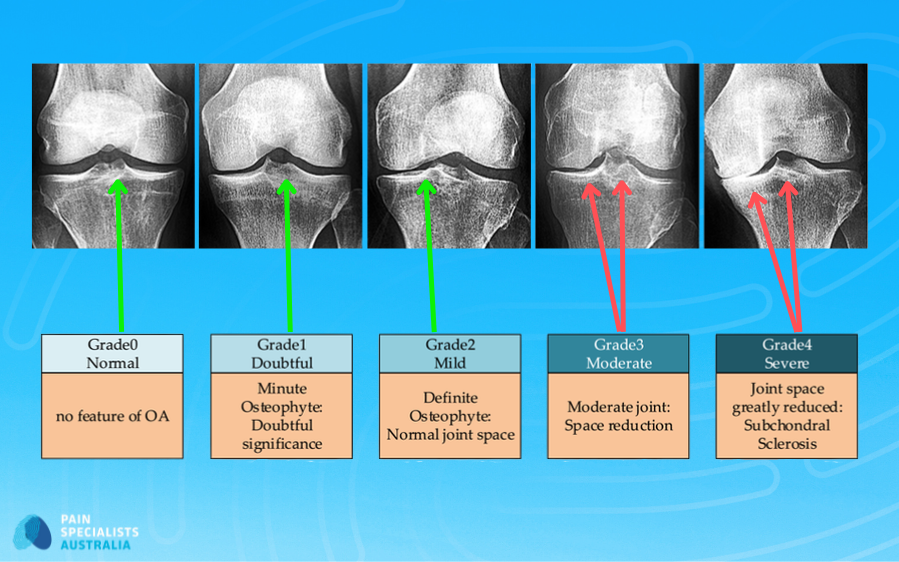
Knee osteoarthritis graded from mild to severe to guide planning.
What do Patients Describe?
We listen closely to what people with knee arthritis share in clinics and online communities. Their stories help shape how we support every new patient. Here is what we hear most often:
“I cannot sleep because my knee throbs at night”
“Stairs and getting up from a chair are painful”
“I feel too young for a knee replacement and told to wait”
“Pain feels worse than the scan report suggests”
“Worry about surgery stories from friends and forums”
These lived experiences remind us why early diagnosis and a structured plan matter. At Pain Specialists Australia, we work to replace fear with understanding, and isolation with coordinated, expert support.
What to expect at your first visit
We start by listening. You complete a short questionnaire so we can map pain to your goals and daily tasks. We examine your knee, strength, and gait. We review any scans you already have. If needed, we order an X-ray and only add an MRI if it will change your care. You leave with a clear treatment plan and a set review date.
Early steps
Lifestyle and activity tweaks that fit your day.
Targeted strength and range of motion work.
Weight support & dietetics if helpful.
Simple pain relief with a flare plan.
Physiotherapy guidance to keep you progressing.
If symptoms persist
Consider a cortisone injection for a flare.
Discuss hyaluronic gel or PRP case by case.
Set expectations on benefit and duration, then review.
Genicular nerve block to test if a nerve ablation will be helpful.
If the block helps, we consider radiofrequency ablation for longer relief.
If pain and disability remain severe
We will coordinate a surgical review at the right time.
We would refer you to some of the leading orthopaedic surgeons in Melbourne and across Australia.
Once a referral is received, our team of nurses and administrative staff contact patients within 24 hours to arrange assessment with one of our Pain Specialists at the most convenient Melbourne location.
Your pathway at Pain Specialists Australia

Your step-by-step plan from first visit to the right next step.
Step 1. Assessment that maps pain to function
We start with your story, goals and daily tasks. We examine strength, movement, sensitivity and alignment. X-rays are used when helpful. MRI is selective and guided by how it will change care. You do not always need an MRI to diagnose knee arthritis.
Step 2. First-line care that works in real life
Targeted strengthening and pacing reduce pain and improve confidence. Sit to stand, step-ups, mini-squats and calf raises are good starts. Short sets most days beat one hard session. Weight support can add extra benefit. We set review points, so progress is clear.

Start with sit to stand, step ups, mini squats and calf raises most days.
Step 3. Injections with clear expectations
People often ask, “how long do knee cortisone injections last” and “are gel injections worth it.” Corticosteroid can help a flare for weeks and sometimes even many months. Hyaluronic gel helps some people and not others. PRP is considered on a case by case basis. If relief is brief, we plan the next step rather than repeat often.
Step 4. Nerve-targeted options
A genicular nerve block for knee pain can be considered. If the block helps, radiofrequency ablation may extend relief in selected patients. It is image-guided and a day procedure. Results vary, so careful selection and follow-up matter.

Genicular nerve ablation targets small pain carrying nerves around the knee.
How long does genicular nerve ablation last?
Relief can last months or even up to a year or two in some selected patients. Duration varies with your pain pattern, strength program and activity load. We begin with a diagnostic block to check likely benefit, then plan ablation if the block helps. We review outcomes at set intervals.
Who is a good candidate for nerve ablation?
Knee osteoarthritis that limits daily life
Short-lived benefit from injections
Positive response to a genicular nerve block
Able to follow a strength and rehab plan
Nerve ablation may be suitable if test/diagnostic injections reduce the pain significantly and/or improve function.
In selected cases, we may add an alcohol neurolytic block to extend pain relief after nerve ablation.
Step 5. When to talk about Knee Replacement
We consider surgery when daily life remains limited after a full non-surgical plan. We help you weigh timing and expectations, then coordinate with your surgeon if it is the right step.
We can refer you to leading orthopaedic surgeons in Melbourne and across Australia when surgery is the best option.
While surgery is successful for many, we also provide specialized support for those who experience chronic pain after knee replacement even when their scans and hardware are technically perfect.
Before committing to surgery, we recommend watching our clinical masterclass on the plumbing vs. wiring of chronic knee pain to understand why some 'perfect' surgeries still result in persistent pain.
This video provides general information only and is not a substitute for individual medical advice. Outcomes and treatment suitability vary. Accessing this content does not establish a doctor-patient relationship. Any case studies mentioned are hypothetical.
WATCH: Understanding the "Success-Pain Gap" Before Surgery
Before committing to a total knee replacement, it is vital to understand why 1 in 5 patients still experience persistent pain after a "perfect" operation. In this clinical masterclass, Dr. Nick Christelis and Dr. Andy Kwok, explain the difference between fixing the joint and treating the nervous system.
This video provides general information only and is not a substitute for individual medical advice. Outcomes and treatment suitability vary. Accessing this content does not establish a doctor-patient relationship. Any case studies mentioned are hypothetical.
Fast-track to the insights you need:
[09:16] Plumbing vs. Wiring: Why a surgeon can fix the "plumbing" (the joint), but the "wiring" (the nerves) can still cause pain.
[13:27] Pre-Op Risk Factors: Learn which biological and lifestyle factors increase the risk of developing chronic pain after surgery.
[14:28] Beyond the X-Ray: Why a SPECT CT scan can be used to locate the hidden inflammation that standard scans miss.
[32:29] The Spine Connection: How your lower back can mimic "bone-on-bone" knee pain, leading to unnecessary surgeries.
[35:12] Genicular Nerve RFA: A non-surgical way to treat pain.
Where GAE fits
Genicular artery embolisation is an emerging option. Early studies suggest improvement for some people. Evidence and protocols are still developing. We are watching this space.
When Knee Pain Doesn’t Improve, Something Is Being Missed
Knee pain that doesn’t improve needs a different approach. Specialists need to do a full assessment and determine what other factors are at play. An example of this would be undiagnosed neuropathic pain (nerve pain) which can be associated with some forms of knee pain.
Neuropathic features in knee arthritis
Not all knee arthritis pain feels the same. A meaningful minority, around 7 to 10 percent, show clear nerve pain (neuropathic) features such as burning, pins and needles, and touch sensitivity. If we suspect nerve pain with our knee pain, we adjust your plan. That can include targeted medicines, nerve-focused procedures, and desensitisation strategies alongside exercise.
If nerve pain is part of the picture, earlier knee treatments may not have helped and can sometimes make the pain worse.
Why choose Pain Specialists Australia
Rapid access to a specialist plan and clear next steps.
Full pathway under one roof, including exercise, medications, injections and nerve procedures.
Senior pain physicians with interventional expertise and hospital access.
Team care with physiotherapy and psychology where helpful.
Review points to avoid drift and repeat short term fixes.
Access to a wide network of senior orthopaedic surgeons.
Once a referral is received, our team of nurses and administrative staff contact patients within 24 hours to arrange assessment at the most convenient Melbourne location.
Costs and rebates in Melbourne
Most assessments and procedures attract Medicare or private health rebates. Out-of-pocket costs vary by hospital and insurer. We provide a written quote before you decide. Ask about costs for knee injections, genicular nerve blocks and genicular ablation at your first visit.
Where we see patients
We assess and treat people across Melbourne and Victoria, including Richmond, Heidelberg, Bayside and nearby suburbs.
Learn more about our full clinical pathway for all forms of knee pain.

Frequently Asked Questions (FAQ)
1. How do you diagnose knee arthritis without overusing scans?
We start with your story and function. Examination comes next. X-rays confirm osteoarthritis when needed. MRI is used when it will change care. If nerve mediated pain is likely, a genicular nerve block can help confirm the driver before longer lasting options. The aim is a clear plan, not only a label.
2. Do cortisone (steroid) knee injections work and how long do they last?
They can help a flare for weeks, sometimes even months. Relief varies from person to person. Injections are paired with exercise and load support. Repeat injections can be considered. We set a review point early and plan what to do next if relief is short.
3. Are gel injections worth trying?
Gel injections for knee arthritis, also called hyaluronic acid, help some people move more easily for a period. Others notice little change. Evidence is mixed. We set clear goals, timing and review points before you choose. If relief is brief, we step up your plan. Gel injections can be costly, so a genicular nerve block or genicular nerve ablation may be alternative options to consider.
4. What is a genicular nerve ablation?
It targets small nerves around the knee that carry pain. We start with a diagnostic block. If that helps, radiofrequency ablation may extend relief in selected patients. It is image guided and a day procedure. Results vary, so selection, exercise and follow-up matter.
5. Is GAE proven?
GAE is still developing. Early reports are promising for some people. More research is underway. Suitability is case by case. Protocols are being developed.
6. What exercises should I start with?
Knee arthritis exercises to start: sit to stand, step-ups, mini-squats and calf raises. Do small sets most days. Progress slowly. A physiotherapy-guided program reduces flare-ups and keeps you moving.
7. Can I drive after a knee injection?
Usually yes after a short observation period if you feel well and your knee is stable. If the injected knee is your driving leg or you feel lightheaded, arrange a ride. Your doctor will advise on the day.
8. How soon can I return to walking after nerve ablation?
Most people walk the same day and resume normal activity in a few days. Keep exercises light in the first week. We will give you a simple plan and follow up routinely.
References
Further Reading and References on Knee Arthritis:
1. Kolasinski SL, Neogi T, Hochberg MC, Oatis C, Guyatt G, Block J, et al. 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2020 Feb;72(2):149-162.
- Core care emphasises education, structured exercise, weight management, topical NSAIDs first line, and short courses of intra-articular steroids for flares.
https://pubmed.ncbi.nlm.nih.gov/31908163/
2. Bannuru RR, Osani MC, Vaysbrot EE, Arden NK, Bennell K, Bierma-Zeinstra SMA, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019 Nov;27(11):1578-1589.
- Patient-centred algorithm prioritising education, exercise, weight loss, and topical NSAIDs; oral NSAIDs and short-term steroid injections reserved for persistent pain.
https://pubmed.ncbi.nlm.nih.gov/31278997/
3. Arden NK, Perry TA, Bannuru RR, Bruyère O, Cooper C, Hofmann-Amtenbrink M, et al. Non-surgical management of knee osteoarthritis. Nat Rev Rheumatol. 2021 Feb;17(2):116-131.
- Consensus across OARSI and ESCEO on education, structured exercise, weight loss and topical NSAIDs as first-line care; clarifies where injections fit.
https://pubmed.ncbi.nlm.nih.gov/33116279/
4. McAlindon TE, LaValley MP, Harvey WF, et al. Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis: a randomised clinical trial. JAMA. 2017 May 16;317(19):1967-1975.
- Repeated triamcinolone caused greater cartilage loss than saline over 2 years with no pain advantage.
https://pubmed.ncbi.nlm.nih.gov/28510679/
5. Deyle GD, Allen CS, Allison SC, et al. Physical therapy versus glucocorticoid injection for osteoarthritis of the knee. N Engl J Med. 2020 Apr 9;382(15):1420-1429.
- At 1 year, physiotherapy produced better pain and function outcomes than a single steroid injection.
https://bookcafe.yuntsg.com/ueditor/jsp/upload/file/20200428/1588060128388051747.pdf
6. Choi WJ, Hwang SJ, Song JG, Leem JG, Kang YU, Park PH, Shin JW. Radiofrequency treatment relieves chronic knee osteoarthritis pain: a double-blind randomised controlled trial. Pain. 2011 Mar;152(3):481-487.
- Genicular nerve radiofrequency neurotomy reduced pain and improved function versus sham in selected OA patients.
https://pubmed.ncbi.nlm.nih.gov/21055873/
7. Zhang H, Li J, Chen M, Zeng C, Li H, Li Y, et al. Efficacy and safety of radiofrequency ablation for treatment of knee osteoarthritis: a meta-analysis of randomised controlled trials. J Int Med Res. 2021;49(4):3000605211006647.
- Pooled RCTs show RFA improves pain and function without higher adverse events versus controls.
https://pubmed.ncbi.nlm.nih.gov/33887985/
8. Liu J, Wang T, Zhu Z-H. Efficacy and safety of radiofrequency treatment for improving knee pain and function in knee osteoarthritis: a meta-analysis of randomised controlled trials. J Orthop Surg Res. 2022 Jan 13;17(1):25.
- Confirms RFA benefits across multiple RCTs; suggests genicular-targeted RFA outperforms intra-articular RF in subgroup analyses.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8760716/
9. Taslakian B, Al-Samman AM, Mashal M, Issa G, Patel IJ, Shuaib W, et al. Embolisation of the genicular arteries for treatment of knee osteoarthritis: review of current evidence and future perspectives. Cardiovasc Intervent Radiol. 2023 Jun;46(6):559-570.
- GAE shows early symptom improvement in cohort studies; evidence base remains limited and longer-term, controlled data are needed.
https://pubmed.ncbi.nlm.nih.gov/36865988/
10. Epelboym Y, Mandell JC, Collins JE, Burch E, Shiang T, Killoran T, Macfarlane L, Guermazi A. Genicular Artery Embolization as a Treatment for Osteoarthritis Related Knee Pain: A Systematic Review and Meta-analysis. Cardiovasc Intervent Radiol. 2023 Jun;46(6):760-769.
- Meta-analysis signals short-term pain relief after GAE with low complication rates; emphasises need for robust RCTs and patient selection.
https://pubmed.ncbi.nlm.nih.gov/36991094/
11. Sabha M, Hochberg MC. Non-surgical management of hip and knee osteoarthritis; comparison of ACR/AF and OARSI 2019 and VA/DoD 2020 guidelines. Osteoarthr Cartil Open. 2021 Dec 25;4(1):100232.
- Cross-guideline synthesis highlighting shared core treatments and where recommendations diverge.
