

Injections for knee pain work best when a diagnosis has been made which allows the injection to target the real cause of persistent pain.
Most people do not start with injections. They reach this point after months or years of knee pain that doesn’t improve. They have tried physiotherapy, exercise programs, medications, pacing, weight loss, and rest.
Then when they get the injections, often they say the same thing. “The injection helped for a bit, then the pain came back.” This pattern is common. It usually means the pain source was never clearly identified.
At Pain Specialists Australia, injections are not offered as a reflex or as the only treatment. Injections are chosen after a thorough medical assessment, examination, scans (in some instances) and review. Injections must form part of a broader treatment plan.
While injections offer powerful relief, they are most effective when used as part of a complete clinical pathway for persistent knee pain.
Key Takeaways
Knee injections depend on the type of pain, not the scan alone.
Cortisone (steroid) and gel injections help flares, not persistent pain.
PRP suits selected tissue-driven knee pain.
Ongoing pain after surgery is often nerve related. It is more common than expected and requires a different strategy.
Radiofrequency and neuromodulation help refractory knee pain.
Why People Search for Knee Injections
People usually search for knee injections when something has failed. Common reasons include:
“My cortisone injection wore off. What’s next?”
“I’ve tried everything and nothing worked.”
“I still have pain after knee replacement.”
“My scan looks mild, but the pain is severe.”
“I just want to walk, sleep, and live normally again.”
These searches are not really about injections. They are about finding a diagnosis and a treatment plan.
First Question – What Type of Knee Pain Is It?
Knee pain does not come from one structure. Treating all knee pain the same leads to failed injections. Pain specialists listen and examine. They look for pain patterns, not labels.
Some knee pain comes from irritated nerves rather than the knee joint itself.
Here are some pain patterns that can help you get the right diagnosis of knee pain:
Joint and Inflammatory Knee Pain
Joint-driven pain often comes from arthritis or inflammation.
People usually describe:
A deep ache inside the knee
Swelling during flares
Stiffness after rest
Pain worse with walking or stairs
Cortisone (steroid) or gel injections may help here. Relief can be months or longer but is usually temporary and needs review.
Nerve-Driven Knee Pain
Nerve pain feels different and is often not considered or missed.
People describe:
Burning or electric pain
Sharp jabs or shocks
Pain from light touch or clothing
Pain worse at night
Pain that does not match scans
Sometimes this can be part of a more serious nerve pain condition like Complex Regional Pain Syndrome (CRPS)
Nerve pain is common after knee surgery. Joint injections rarely help in these cases.
Tendon and Bursa-Related Knee Pain
Some knee pain comes from the surrounding soft tissue rather than the joint.
This may include:
Pes anserine bursitis
Localised inner knee pain
Pain with specific movements
Targeted injections may help when the diagnosis is clear.
Muscular and Myofascial Knee Pain
Some knee pain comes from the surrounding muscles rather than the joint or nerves.
This often follows:
A strain or overload
Sudden increase in walking or running
Weakness after surgery or injury
Poor movement patterns
People often describe:
Aching around the knee rather than inside it
Pain worse after activity
Tightness or cramping
Pain that changes with position or fatigue
Muscular pain can amplify and worsen other knee problems.
Injections aimed at the joint alone often fail when muscle load is the main driver.
Treatment focuses on:
Correct diagnosis first and foremost
Targeted strength and rehabilitation
Addressing overload rather than masking pain
Referred Knee Pain From the Hip, Spine, or Ankle
Pain from the lower back can sometimes be felt as knee pain.
Not all knee pain starts in the knee. Pain can be referred from nearby joints or the spine.
Common sources include:
Hip joint arthritis
Lumbar spine nerve irritation
Ankle or foot mechanics altering load
Leg length or gait changes
People often say:
“My knee hurts but the knee scans look fine”
“The pain moves”
“Treating the knee didn’t help”
In these cases, knee injections alone rarely solve the problem. The knee becomes the victim, not the cause. Assessment looks beyond the knee to find the true driver of pain.
Multiple Pain Sources Can Exist in the Same Knee
Remember that many knees do not have a single diagnosis. It is common for more than one pain source to exist at the same time.
For example, this may occur in and around a single joint:
Arthritis inside the joint
Nerve pain around the knee
Muscle overload or weakness
Pain referred from the hip or spine
Sensitisation after surgery or an injury
People often say:
“Some pain improved, but not all of it”
“The pain changed after treatment”
“One injection helped one part, not another”
When only one source is treated, pain often persists. This is why chronic knee pain needs expert assessment. A pain specialist looks at how multiple pain drivers interact.
Effective treatment often involves:
Prioritising the dominant pain source
Treating more than one mechanism over time
Reviewing response rather than repeating the same injection
This approach is rarely offered in single-focus clinics.
Watch: Why the "Perfect" Surgery Doesn't Stop the Pain
If your joint replacement is structurally sound but the pain won't settle, you are likely part of the "20% Club." In this video, Dr. Nick Christelis explains why we must treat the "wiring" (nerves) when the "plumbing" (the joint) is already fixed.
This video provides general information only and is not a substitute for individual medical advice. Outcomes and treatment suitability vary. Accessing this content does not establish a doctor-patient relationship. Any case studies mentioned are hypothetical.
Key Insights:
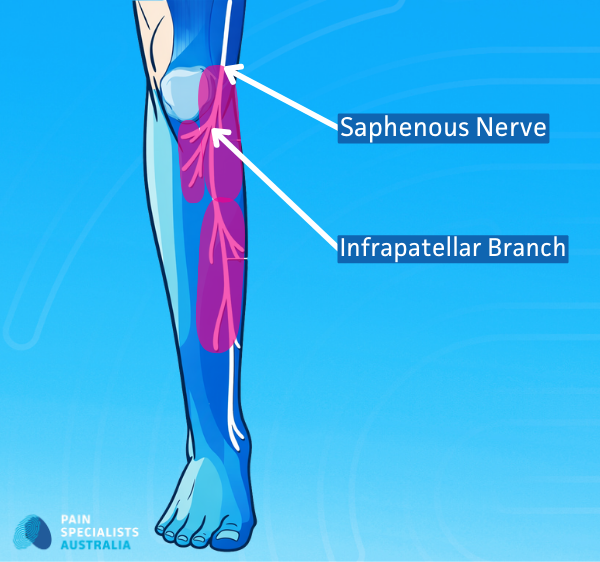
The Saphenous Nerve: Why this nerve is the primary culprit for inner knee burning.
Diagnostic Blocks: How we use precise injections to "test" if a nerve is the true pain generator.
Sarah's Story: A real-world example of moving from chronic post-op pain to a functional life.
Why Knee Injections Fail Even When Scans Look Mild or Even Normal
This is one of the most common frustrations people describe.
They are told:
“The MRI looks fine.”
“The X-ray shows mild arthritis.”
“Nothing serious is wrong.”
Yet the pain is severe. Scans only show structure. They do not show nerve sensitivity, pain signalling, or sensitisation. This key in these complex clinical situations is to correlate the clinical situation and circumstance with the scans or imaging results.
Common reasons injections fail include:
Pain is nerve-driven, not inflammatory
Pain comes from outside the joint
Sensitisation of nerves after surgery or injury
Referred pain from higher nerve levels
This is why diagnosis matters more than images.
Cortisone Injections for Knee Pain
Cortisone (steroid) injections aim to reduce inflammation. They are often the first injection people try.
When Cortisone (Steroid) Can Help
Cortisone may help when:
The knee is swollen
Pain has recently flared
Inflammation limits movement
Arthritis is mild to moderate
Relief may last weeks or months.
Why Cortisone (Steroids) Often Stops Working
Many people say, “It worked, then the pain came back.”
Common reasons include:
Pain is nerve-driven
Arthritis is advanced
Repeated injections lose effect
Movement and load issues persist
Repeating cortisone without a new plan rarely helps.
Targeted injections provide a vital window of relief for patients seeking effective knee arthritis and osteoarthritis treatment in Melbourne without immediate surgery.
Gel Injections for Knee Pain
Gel injections aim to improve joint movement by acting as a joint lubricant.
Some people notice:
Less stiffness
Easier movement for a time
Others feel little change.
Gel injections may suit:
Early to moderate arthritis
People delaying surgery
Those who cannot tolerate cortisone
They do not treat nerve pain.
Knee injections work best when used within a structured treatment plan.
Platelet Rich Plasma (PRP) and Biologic Injections for Knee Pain
PRP injections use concentrated components from your own blood. The aim is not to numb pain or reduce inflammation quickly. The aim is to support tissue healing and improve how the knee tolerates load.
PRP works by:
Delivering growth factors to stressed tissue
Supporting tendon, ligament, and cartilage health
Reducing pain over time rather than immediately
People often choose PRP because they want:
A non-surgical option
A more biological approach
Support for early joint or tendon changes
An option when cortisone relief was short-lived
PRP is not a painkiller. Pain relief, when it occurs, builds gradually over weeks to months.
What PRP Is Designed to Treat
PRP may help when:
Pain is tissue-driven
Arthritis is early
Tendon or ligament pain dominates
A gradual approach is acceptable
PRP works slowly. Results vary between people. PRP is considered a safe treatment.
Where PRP Is Less Likely to Help
PRP is less effective when:
Arthritis is severe
Pain is nerve-based
Pain follows knee replacement
Rapid relief is needed
PRP should always be discussed honestly and form part of a more broader treatment plan.
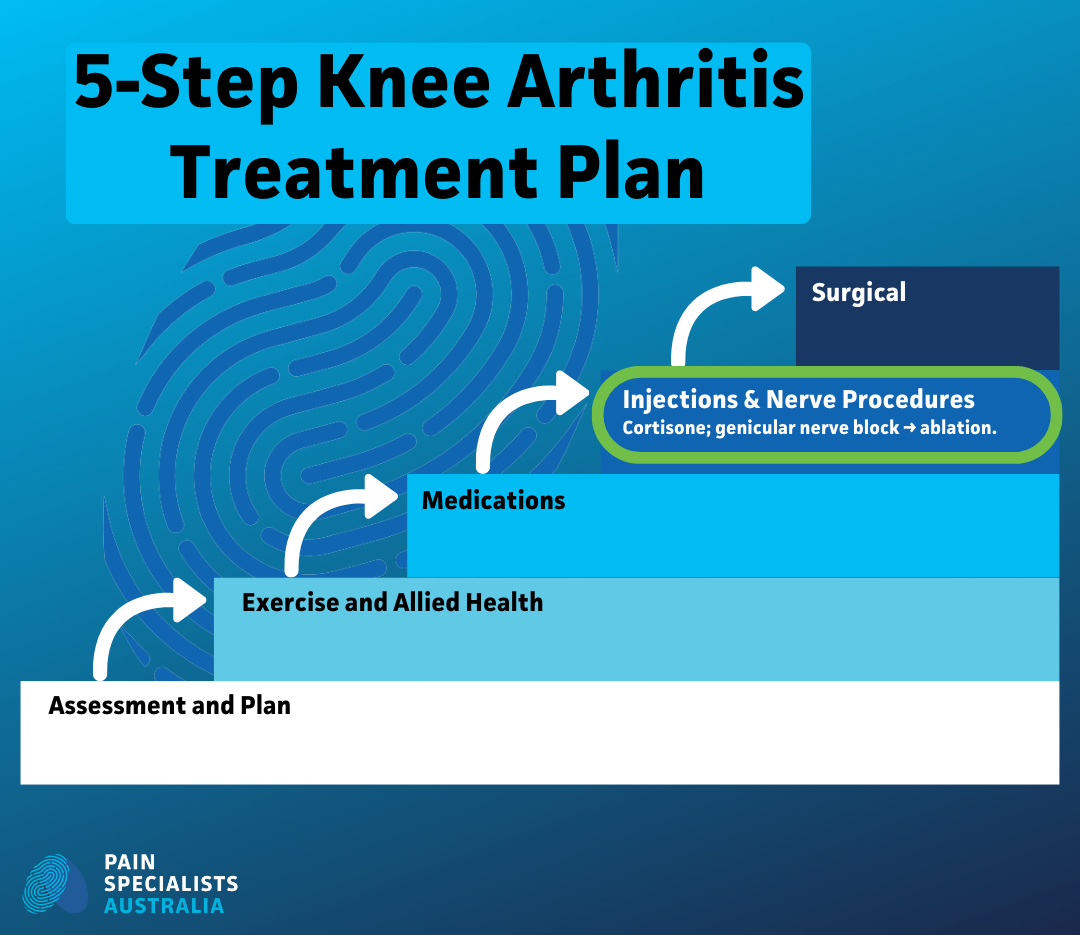
Nerve-Targeted Injections for Knee Pain
Nerve-targeted treatments matter when pain persists. This is often when people say, “Nothing worked.”

Genicular nerve procedures are performed using imaging to precisely target pain pathways around the knee.
Genicular Nerve Blocks
Genicular nerve blocks act as test injections. They help answer a key question: Is the pain being driven by nerves around the knee?
Short-term relief suggests the nerve is involved.
That information guides treatment decisions.
We also use these diagnostic blocks to identify the biological cause of chronic pain after knee replacement when scans show the hardware is stable
Genicular Nerve Radiofrequency
Radiofrequency reduces pain signalling from nerves.
It may help when:
Arthritis pain persists
Joint replacement surgery needs to be delayed or avoided
Pain continues after knee replacement
Diagnostic blocks were helpful but short-lived
Length of relief is aimed to last months and years but the time can be variable.
Pulsed Radiofrequency of Peripheral Knee Nerves
Pulsed radiofrequency is an injection technique that suppresses and modulates nerve activity. It does not destroy the nerve(s).
It suits:
Burning or electric pain
Sensory-dominant pain
Post-surgical knee pain
Cases where nerve preservation matters
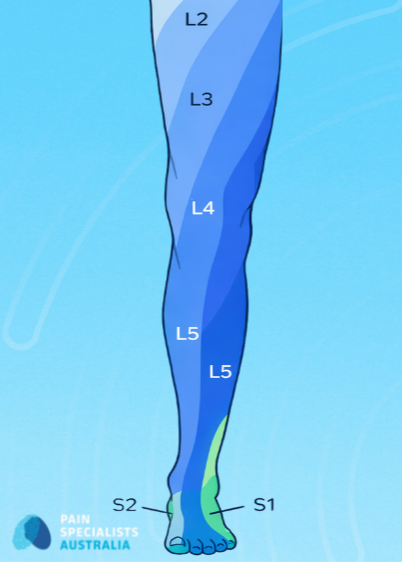
L3 and L4 Nerve Targeting for Refractory Knee Pain
Some knee pain is referred from higher nerve pathways.
L3 and L4 nerves are the sensory nerves of the knee and in some instances these nerves can be targeted to treat knee pain.
Targeting these nerves may help when:
Knee injections failed
Pain spreads beyond the joint
Surgery did not resolve pain
Pain feels deep or poorly localised
This approach requires specialist assessment and expertise.
If your pain feels like burning or electrical zaps, our injections focus on specialised nerve pain treatment to reset the overactive signals.
Alcohol Neurolytic Blocks for Severe Knee Pain
Alcohol neurolytic blocks are selective treatments. They reduce nerve function using alcohol instead of heat, offering another option when radiofrequency is not suitable or trialled and not long-lasting.
They may suit:
Severe arthritis
Non-surgical candidates
End-stage pain where durability matters
They are not routine injections. They should be used carefully and should only be done by experienced specialists.
Chronic Pain After Knee Replacement
Ongoing pain after knee replacement is more common than expected. Many people are told the surgery was successful and the scans look fine, but the pain continues or some. In some instances, if carefully assessed the knee joint pain disappears after the joint replacement and is replaced with new/worse nerve (neuropathic) pain.
Pain after knee replacement is often nerve-driven.
Why Pain Persists After Surgery
Pain may persist due to:
Nerve irritation or injury
Sensitisation of the nervous system
Scar-related nerve pain
Referred pain patterns
Standard scans do not show nerve pain.
Saphenous and Infrapatellar Nerve Pain
This is a common type of nerve pain that might occur after knee replacement. Inner knee burning pain often involves the saphenous nerve and or the infrapatellar nerve.
People describe:
Sharp inner knee pain
Pain from light touch
Pain worse at night
Poor sleep and fatigue
Targeted nerve treatments may help.
Deep Dive: The Clinical Masterclass on Knee Wiring
This episode of The Pain Diaries Podcast explores how we treat complex knee pain. We look beyond the joint to find the true source of your discomfort. Dr. Nick Christelis and Dr. Andy Kwok explain how we "reset" a sensitised nervous system after knee replacement surgery using advanced medical pathways.
This video provides general information only and is not a substitute for individual medical advice. Outcomes and treatment suitability vary. Accessing this content does not establish a doctor-patient relationship. Any case studies mentioned are hypothetical.
Fast-track to the technical answers:
[09:16] Plumbing vs. Wiring: Why your scans look fine while the pain is severe.
[20:53] Topical Compound Creams: How specialized Ketamine and Clonidine creams quieten overactive skin nerves.
[32:29] The Spine Connection: How to tell if knee pain is actually coming from your back.
[35:12] Genicular Nerve RFA: Using thermal energy to safely interrupt pain signals.
[46:16] The Nervous System Reset: Can you retrain your brain to stop producing pain after surgery?
When Injections Work Best
Injections work best when part of bigger and more structured treatment plan.
A plan may include:
Movement retraining
Load management
Strength and stability work
Pain education
Medications that target the specific pain
Clear review points
Endless injections without progress do not help.
Neuromodulation for Severe Refractory Knee Pain
Neuromodulation uses targeted electrical or drug-based therapies to reduce pain signals when other knee treatments have failed.
Some people reach a point where:
Surgery is not needed
Surgery is complete
No further surgery is advised
Pain still dominates daily life
In these cases, neuromodulation may be considered.
Peripheral Nerve Stimulation for Knee Pain
Nerve stimulation targets pain signals directly.
It may help when:
Pain is nerve-driven
Injections gave short relief
Pain persists after surgery
Medication options are limited
Stimulation aims to reduce pain without destroying nerves.
Intrathecal Drug Delivery for Complex Knee Pain
Intrathecal therapy delivers medication directly to the spinal fluid.
It may suit:
Severe, widespread pain
High medication side effects
Complex pain after multiple treatments
This is reserved for carefully selected cases and should be performed by experts and experienced specialists.
Injection Comparison at a Glance

Click the table to enlarge.
Why Choose Pain Specialists Australia?
Many people come to us after years of frustration and no help with past treatments.
Our approach focuses on:
Diagnosis of the pain before procedures
Matching treatment to pain type
Full interventional expertise
Experience with post-surgical knee pain
Once a referral is received, our team of nurses and administrative staff contact patients within 24 hours to arrange assessment at the most convenient Melbourne location. Our locations are Central (Richmond), North (Heidelberg), and South (Bayside).
What Patients Describe
We listen closely to what people with knee pain share in clinics and online communities.
Common themes include:
Short relief, then pain returns
Still in pain after surgery
No explanation for failed injections
Feeling dismissed or stuck
Wanting a clear plan
These experiences guide patients to our clinic and our experienced pain specialists.
Frequently Asked Questions

1. Do knee injections work better than surgery?
Injections and surgery treat different problems. Injections aim to reduce pain and improve function. Surgery changes joint structure. Many people use injections to delay surgery or manage pain after surgery. The right option depends on diagnosis, not scan severity alone.
2. Can nerve blocks help pain after knee replacement?
Yes. Persistent pain after knee replacement is common and often nerve-driven. Genicular or saphenous nerve blocks can identify whether nerves are the main pain source. If blocks help, longer-lasting options may be considered.
3. Is pulsed radiofrequency safer than nerve ablation?
Pulsed radiofrequency does not destroy nerves. It modulates nerve signalling and suits burning or electric pain. It is often used when nerve pain dominates and preservation of sensation matters.
4. Does PRP work for knee arthritis?
PRP may help selected people with tissue-driven pain and early arthritis. It is less effective for severe arthritis or nerve pain. Results vary, and it works best as part of a broader plan.
5. How many knee injections can you safely have?
There is no single number. Safety depends on injection type, spacing, and your health. Repeating injections without benefit is rarely helpful. Review is essential if relief is short-lived.
References
Further Reading and References on Knee Injections:
1. McAlindon TE, Bannuru RR, Sullivan MC, Arden NK, Berenbaum F, Bierma-Zeinstra SM, et al.OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis and Cartilage. 2014 Mar;22(3):363–388.
These international guidelines outline evidence-based use of knee injections, exercise, and non-surgical treatments, highlighting where injections are appropriate and where benefits are limited.
https://pubmed.ncbi.nlm.nih.gov/24462672/
2. Bannuru RR, Osani MC, Vaysbrot EE, Arden NK, Bennell K, Bierma-Zeinstra SMA, et al. Comparative effectiveness of pharmacologic interventions for knee osteoarthritis: a systematic review and network meta-analysis. Annals of Internal Medicine. 2015 Jul 7;162(1):46–54.
This large meta-analysis compares cortisone, hyaluronic acid, and PRP injections, showing variable short- and medium-term benefits and reinforcing the need for patient selection.
https://pubmed.ncbi.nlm.nih.gov/25560713/
3. Choi WJ, Hwang SJ, Song JG, Leem JG, Kang YU, Park PH, Shin JW. Radiofrequency treatment relieves chronic knee osteoarthritis pain: a double-blind randomized controlled trial. Pain. 2011 Mar;152(3):481–487.
This landmark trial demonstrates that genicular nerve radiofrequency can significantly reduce pain in knee osteoarthritis compared with sham treatment.
https://pubmed.ncbi.nlm.nih.gov/21055873/
4. Ikeuchi M, Ushida T, Izumi M, Tani T. Percutaneous radiofrequency treatment for refractory anteromedial pain of osteoarthritic knees. Pain Medicine. 2011 Apr;12(4):546–551.
This study supports nerve-based radiofrequency treatment for chronic knee pain when conventional injections and conservative care have failed.
https://pubmed.ncbi.nlm.nih.gov/21463469/
5. Abd-Elsayed A, Anis A, Kaye AD. Radio Frequency Ablation and Pulsed Radiofrequency for Treating Peripheral Neuralgias. Curr Pain Headache Rep. 2018 Jan 25;22(1):5.
This review explains how pulsed radiofrequency modulates nerve signalling without destroying nerves, making it suitable for neuropathic and post-surgical pain.
https://pubmed.ncbi.nlm.nih.gov/29372343/
6. Schmidt PC, Ruchelli G, Mackey SC, Carroll IR. Perioperative gabapentinoids: choice of agent, dose, timing, and effects on chronic postsurgical pain. Anesthesiology. 2013 Nov;119(5):1215-21.
This paper highlights mechanisms of chronic pain after surgery, including nerve sensitisation, which helps explain persistent pain after total knee arthroplasty.
https://pubmed.ncbi.nlm.nih.gov/24051389/
7. Trescot AM. Cryoanalgesia in interventional pain management. Pain Physician. 2003 Apr;6(3):345–360.
This review covers chemical and physical neurolytic techniques, including alcohol neurolysis, as options for reducing nerve function in severe, refractory pain.
