
Treatment for pain after spinal fusion helps patients find answers when surgery has not brought the relief they expected. Many people continue to feel significant discomfort long after their bones have fused. You might feel frustrated if your surgeon says the hardware looks perfect. You may wonder why your life has not returned to normal. Our team understands that a successful surgery does not always mean the pain is gone. We look beyond the metal and bone to find the biological source of your distress.
Key Takeaways
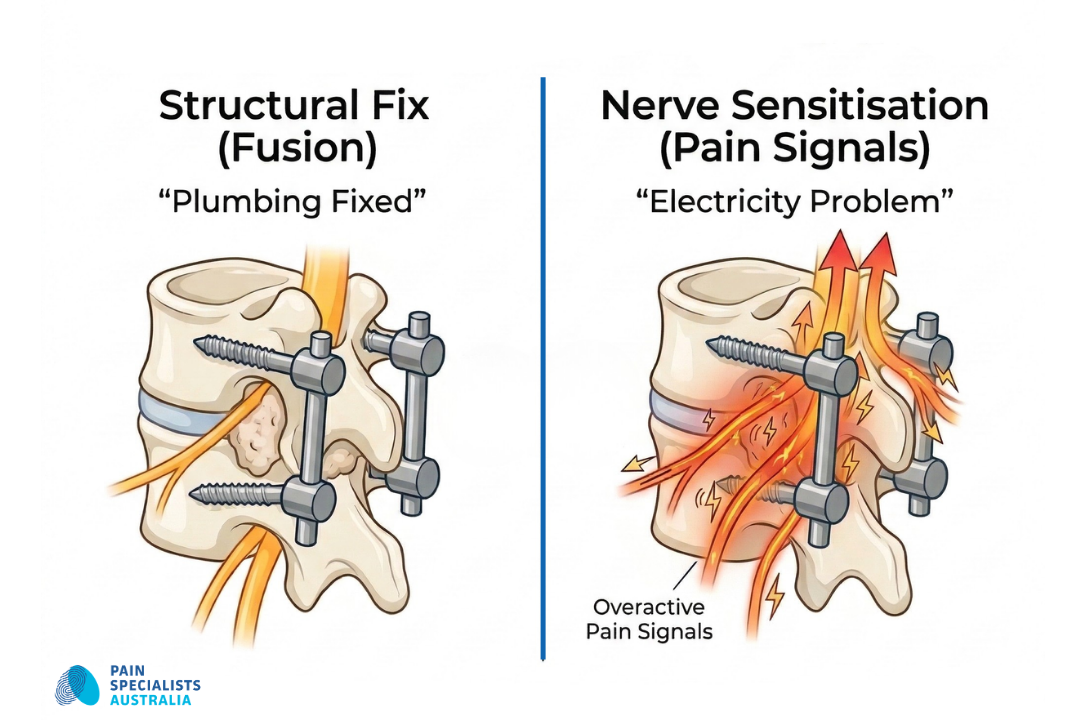
Hardware vs Biology: A solid fusion means the bone has healed, but the nerves may still be sensitised.
Scar Tissue Matters: Adhesions (scar tissue) can tether nerves near the fusion site and cause burning pain.
The Level Above: Pain often shifts to the joint above the fusion. Doctors call the condition Adjacent Segment Disease.
The SI Joint Factor: Fusing the spine changes how you move. The change often puts new stress on the sacroiliac (SI) joints.
Beyond the X-ray: Clear scans do not mean the pain is not real. We study how your nerves function. We look beyond how the bone looks.
When the Hardware is Perfect, but the Pain is Not
It is common to hear that your surgery was a technical success. Surgeons often point to a solid bone bridge and secure screws on a scan. Yet, you might still feel a deep, aching heaviness in your back that makes every step a challenge.
Patients often describe a sensation like a cold metal crowbar is lodged in the spine. You may feel betrayal when a doctor says the hardware is fine while you struggle to walk or sit. At our Richmond and Heidelberg and Bayside clinics, we look past the metal.
We focus on the biology of the nerves surrounding the fusion site rather than just the structural appearance of the bone.
While a surgeon ensures the spine is structurally sound, we focus on the biological response. In this episode of The Pain Diaries Podcast, Melbourne Neurosurgeon Dr Jeremy Russell joins Dr Nick Christelis to discuss why even a “perfect” surgery can sometimes leave a patient with persistent pain.
Expert Insight: Neurosurgeon Dr Jeremy Russell and Dr Nick Christelis discuss why clinical logic must go beyond the scan to find the true generator of post-fusion pain.
This video provides general information only and is not a substitute for individual medical advice. Outcomes and treatment suitability vary. Accessing this content does not establish a doctor-patient relationship. Any case studies mentioned are hypothetical.
What Patients Describe: The Voice of Chronic Pain
We listen closely to what people with chronic spinal pain share in clinics and online communities. Their stories help shape how we support every new patient. Here is what we hear most often:
The "Crowbar" Sensation
Many patients report a deep, heavy feeling in the lower back. Some compare the sensation to a cold crowbar lodged in the spine. The mechanical restriction makes bending or twisting feel impossible. You may feel like your back is permanently encased in concrete.
Burning and Electric Shocks
Nerve pain often feels like walking on hot coals. You might experience sharp lightning bolts that shoot down your legs. The signals happen without warning and can make walking difficult. These sensations suggest that the nerves are in a state of high alarm.
The "Perfect Scan" Frustration
The emotional toll of persistent pain is heavy. Surgeons often tell patients that the X-ray or MRI looks perfect. You might feel like your experience is being dismissed. We know that a normal scan does not mean you are imagining the pain.
It is a clinical paradox: the hardware is solid, yet the nerves are screaming. This detailed discussion explains the mismatch between what your X-ray shows and what your body feels, and why the answer lies in the micro-environment of the nerves, not more surgery.
This video provides general information only and is not a substitute for individual medical advice. Outcomes and treatment suitability vary. Accessing this content does not establish a doctor-patient relationship. Any case studies mentioned are hypothetical.
Nerve Sensitisation and Spinal Fusion Hardware
Why Does It Still Hurt? The Main Drivers Of Fusion Pain
A spinal fusion fixes the structure of your back. However, the procedure does not always fix the biological environment of your nerves. We focus on three main reasons for ongoing pain.
Epidural Fibrosis (Internal Scarring)
Scar tissue naturally forms after any surgery. In some cases, the tissue grows too thick around the nerve roots. The scarring acts like duct tape and tethers the nerves to the surrounding bone. When you move, the tissue pulls on the nerves and causes a burning sensation.
Nerve Sensitisation
Nerves can stay in a state of alarm even after the original pressure is gone. The nervous system remembers the pain from before your surgery. Doctors call the state nerve sensitisation. The nerves become so sensitive that even light touch or movement causes a sharp response. This is a feature of nerve pain (neuropathic pain).
The Domino Effect (Adjacent Segment Disease)
A fusion stops movement at one or more levels of your spine. The lack of movement forces the joints above and below to work much harder. The extra stress can lead to rapid wear and tear in those areas. You might feel new pain just above where the rods and screws end.
Sacroiliac Joint Overload
A fusion changes how the spine moves. The sacroiliac joints must absorb more stress. Over time they can become inflamed and painful.
Fusing one level of the spine changes the load on the segments above and below. We call this Adjacent Segment Disease. Watch our specialists explain the 'secrets' to relieving this specific type of post-surgical pain without resorting to further fusion.
This video provides general information only and is not a substitute for individual medical advice. Outcomes and treatment suitability vary. Accessing this content does not establish a doctor-patient relationship. Any case studies mentioned are hypothetical.
Why Choose Pain Specialists Australia for Post-Fusion Care
Once a referral is received, our team of nurses and administrative staff contact patients within 24 hours to arrange assessment at the most convenient Melbourne location. Our clinic serves as the last stop for patients who have exhausted surgical options. We offer a different perspective on chronic spinal pain.
We Find the True Pain Generator
We offer insight over injections. Standard scans miss the electrical and biological signals of your nerves.
Our specialists use clinical logic and diagnostic blocks to pinpoint the exact source of your pain.
We do not guess; we investigate.

Multidisciplinary Treatment Pathways
We provide pathways over pills.
Managing complex pain requires more than just a prescription. Our team includes FFPMANZCA pain specialists, nurses, physios, psychologists who work together on your plan. We combine medical interventions with physical restoration and education.
A Tier 1 Accredited Team
Our specialists are national leaders in interventional pain medicine. We are a Tier 1 accredited training site. The status means we follow the highest ethics and clinical standards in Australia. You receive care from experts who teach and examine other doctors.
The PSA Pathway to Recovery
We offer advanced options for patients who were told to just live with the pain. Our treatments target the biology of your spine.
If you are experiencing burning, shooting, or electric-style pain after surgery, it may be due to nerve sensitisation or internal scar tissue. Hear our clinical team explain why these biological drivers occur and how we identify them.
This video provides general information only and is not a substitute for individual medical advice. Outcomes and treatment suitability vary. Accessing this content does not establish a doctor-patient relationship. Any case studies mentioned are hypothetical.
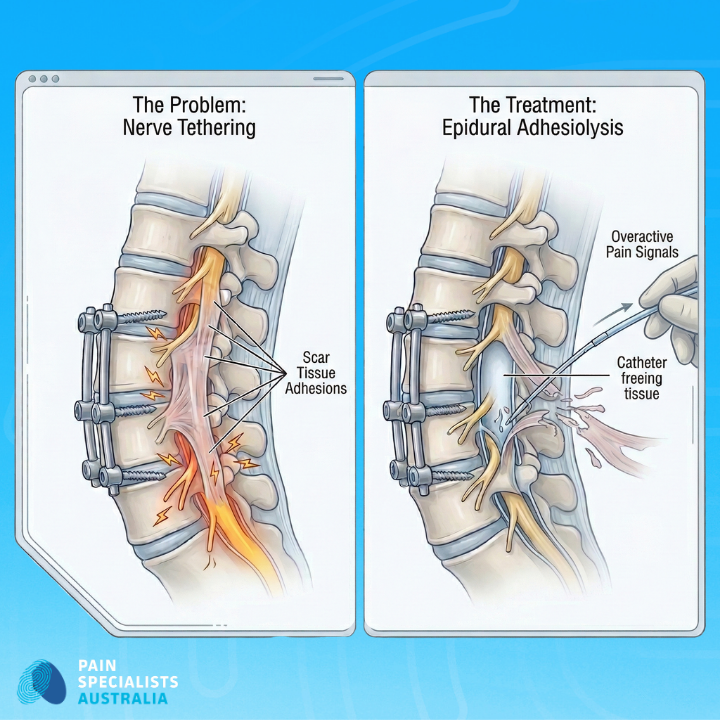
Epidural Adhesiolysis for Post-Surgical Scar Tissue
Epidural Adhesiolysis helps manage the "duct tape" effect of scar tissue. We use a specialised catheter to gently free tethered nerves. The procedure can reduce the burning and pulling sensations you feel during movement.
Neuromodulation acts like a volume control for your nervous system. The technology uses targeted medication or small electrical signals to block pain messages before they reach the brain. It is an effective option for persistent leg and back pain when medications fail.
Serving the Melbourne Health Network
Our clinic is conveniently located in Richmond with satellite locations in Heidelberg and Bayside.
Our specialists regularly collaborate with referring specialists like neurosurgeons and spine surgeons across Melbourne to support complex recovery cases for patients across Victoria.
Frequently Asked Questions

1. Why is my pain worse now than before my spinal fusion?
Pain can increase after surgery due to biological changes. Scar tissue can tether nerves. The nervous system may also become hyper-sensitive. Our specialists look for the biological triggers that scans often miss.
2. My surgeon says the MRI looks perfect. Why am I still in pain?
An MRI shows the structure of your bones and hardware. The scan does not show how your nerves are firing. You can have a perfect mechanical result but still experience significant nerve pain. We focus on how your nerves function.
3. Can my body reject the titanium rods and screws?
True rejection of spinal hardware is rare. Most hardware pain is actually caused by the way the metal interacts with the surrounding structure and nerves. We use diagnostic blocks to see if the hardware is the true source of your discomfort.
4. What is Adjacent Segment Disease?
A fusion stops movement at one level of the spine. The joints above and below must then work harder to compensate. The increased stress can lead to new pain in those areas over time.
5. Is there hope if my surgeon says there is nothing more they can do?
Yes. Surgeons focus on structural fixes. As interventional pain specialists, we support your surgeons and focus on the nervous system. We offer advanced pathways like pulsed radiofrequency and neuromodulation for patients who have exhausted surgical options including those seeking specialised care for pain after laminectomy.
References
Why it Matters for Recovery
Clinical research helps us understand the biology of persistent pain. Evidence shows that scar tissue and nerve sensitisation are major pain drivers. Understanding the factors allows us to offer targeted treatments instead of general advice.
1. Christelis N, et al. Persistent Spinal Pain Syndrome: A Proposal for Failed Back Surgery Syndrome and ICD-11. Pain Medicine. 2021 Apr 20;22(4):807-818. doi: 10.1093/pm/pnab015.
This paper proposes replacing the term “Failed Back Surgery Syndrome” with “Persistent Spinal Pain Syndrome” and outlines how the new term can be integrated into ICD11. The authors argue that the updated terminology better reflects the chronic pain biology and improves clinical communication and classification.
https://pubmed.ncbi.nlm.nih.gov/33779730/
2. Manchikanti L, Manchikanti KN, Gharibo CG, Kaye AD. Efficacy of Percutaneous Adhesiolysis in the Treatment of Lumbar Post Surgery Syndrome. Anesth Pain Med. 2016;6(2):e26172. Published 2016 Mar 7. doi:10.5812/aapm.26172v2
This systematic review concludes that percutaneous adhesiolysis is effective for managing lumbar postsurgery syndrome in patients who have failed conservative treatments including epidural injections. The evidence supports clinically meaningful pain relief and functional improvement in this population.
https://pubmed.ncbi.nlm.nih.gov/27574583/
3. Nissen M, Ikäheimo TM, Huttunen J, Leinonen V, von Und Zu Fraunberg M. Long-Term Outcome of Spinal Cord Stimulation in Failed Back Surgery Syndrome: 20 Years of Experience With 224 Consecutive Patients. Neurosurgery. 2019;84(5):1011-1018. doi:10.1093/neuros/nyy194
This 20-year cohort study shows that spinal cord stimulation can provide good long-term outcomes for many patients with failed back surgery syndrome, with a substantial proportion maintaining satisfactory pain relief and device use over years. The authors note that optimising patient selection could further improve results
https://pubmed.ncbi.nlm.nih.gov/29788145/
4. Tobert DG, Antoci V, Patel SP, Saadat E, Bono CM. Adjacent Segment Disease in the Cervical and Lumbar Spine. Clin Spine Surg. 2017;30(3):94-101. doi:10.1097/BSD.0000000000000442
This paper reviews adjacent segment degeneration after lumbar fusion and highlights that segments next to a fusion construct are at risk of symptomatic degeneration over time. The authors report predicted rates of additional surgery at adjacent levels of roughly 16.5% at 5 years and 36.1% at 10 years.
https://pubmed.ncbi.nlm.nih.gov/27642820/
5. DePalma MJ, Ketchum JM, Saullo TR. Etiology of chronic low back pain in patients having undergone lumbar fusion. Pain Med. 2011;12(5):732-739. doi:10.1111/j.1526-4637.2011.01098.x
Using controlled diagnostic blocks, this study found that the sacroiliac joint is the most common pain generator in patients with chronic low back pain after lumbar fusion. Internal disc disruption, zygapophysial joint pain, and irritation from fusion hardware were less frequent but still important sources.
https://pubmed.ncbi.nlm.nih.gov/21481166/
6. Lewik, Guido et al. “Postoperative Epidural Fibrosis: Challenges and Opportunities - A Review.” Spine Surg Relat Spine surgery and related research vol. 8,2 133-142. 4 Sep. 2023, doi:10.22603/ssrr.2023-0106
This review explores how postoperative epidural fibrosis (internal scar tissue) serves as a primary driver of failed back surgery syndrome by tethering and compressing nerves within the spinal space. It highlights that while traditional imaging often fails to detect these adhesions, advanced interventional strategies like epiduroscopy and adhesiolysis offer promising pathways for addressing the biological causes of persistent pain.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11007250/
7. Gatchel RJ, McGeary DD, McGeary CA, Lippe B. Interdisciplinary chronic pain management: past, present, and future. Am Psychol. 2014;69(2):119-130. doi:10.1037/a0035514
This review synthesises evidence showing that interdisciplinary programs combining medical, physical, and psychological interventions yield better outcomes than single-modality care for chronic pain. The authors emphasise functional restoration, reduced disability, and cost-effectiveness as key advantages of team-based management.

