

Knee Replacement Pain that Won’t Go Away: Why A "Perfect" Scan Still Hurts
Chronic pain after knee replacement is a common challenge where "perfect" surgery still hurts.
You may have been told your X-ray looks perfect and the implant is stable. But your knee still burns, aches, or feels tight. This is where many people get stuck.
Many people start to wonder if something has gone wrong with the surgery, even when they are told everything looks fine.
A normal scan does not mean a normal pain system. In many cases, this is not a joint problem. It is a nerve problem.
What You Need to Know
Up to 1 in 5 patients struggle with persistent pain or chronic pain after a total knee replacement.
A "perfect" X-ray does not explain ongoing pain.
Burning, tight, or sensitive pain often points to nerve involvement.
Diagnosis must identify the exact pain source before treatment.
Ongoing pain is often a biological issue involving nerve sensitivity rather than a mechanical failure.
Targeted nerve treatment can reduce pain and restore function.
First Steps: Ruling Out Surgical Complications
A successful recovery starts with clear communication between the patient and the surgeon. Before pain treatment starts, your surgeon must first rule out surgical problems that may need urgent treatment.
Mechanical knee problems include:
Infection
Loosening of the implant
Instability
Stiffness
Fracture, or
Another structural problem.
If the implant is stable and the operation looks sound, but pain continues, the focus needs to shift.
Pain specialists look beyond hardware to identify nerve irritation, sensitisation, scar-related pain, or inflammation.
What People Describe
We listen closely to what people with persistent knee pain share in clinics and online communities. Lived experiences help shape how we support every new patient. Here is a summary of common complaints:
“I was told everything looks fine, but I’m in more pain than before surgery”
“The pain is worse at night and I cannot sleep”
“Physio is not helping and no one can explain why”
“It feels like something is wrong, but scans say nothing is wrong”
I have a sensation of a tight, vice-like band around the joint.”
“There are burning pains or electrical zaps, often worse at night.
Patient patterns matter because they signal nerve pain rather than slow recovery. Early diagnosis helps guide more targeted care.
Recognising the Symptoms of Nerve Sensitivity
Most ongoing pain after knee replacement is not coming from the implant. It is coming from irritated or sensitised nerves around the knee.
Because post-surgical pain is often a biological issue rather than a joint failure, we use specialized nerve pain treatment protocols to quieten overactive signals and reset the nervous system.
Persistent pain after a knee replacement often presents with distinctive physical signs. The sensation often feels burning, sharp, or sensitive despite normal imaging results. Common signs of post-surgical nerve sensitivity include:
A burning or searing sensation that worsens when resting or at night.
Extreme sensitivity to light touch or the feeling of clothing against the skin.
Sharp, electrical shocks or "zaps" that occur without warning.
A feeling of numbness or "pins and needles" around the surgical scar.
Changes in skin temperature or colour around the knee joint.
Scar tenderness or pain when the scar area is touched.
Persistent pain after knee replacement is part of a larger pattern seen across many types of surgery. You can explore this in more detail in our guide on why pain persists after surgery.
How Do You Actually Find the Cause of Pain?
Standard scans often do not show the true source of pain.
The most reliable way to identify the cause is through targeted diagnostic blocks.
These involve numbing specific nerves to see if the pain improves.
This is often the first time patients get a clear answer about where their pain is coming from.
This step confirms whether the pain is coming from the joint, scar tissue, or specific nerve branches.
Effective pain management requires an accurate diagnosis before any intervention begins. General treatments are often offered before identifying the true source of pain.
At Pain Specialists Australia, we focus on finding the exact pain generator before recommending procedures or medication.
Vague diagnoses often lead to vague and ineffective treatments. Assessment confirms if pain stems from knee nerves, scar tissue, sensitisation, inflammation, or the spine.
Once the pain source is clear, treatment can be more precise and more effective.
A structured treatment pathway replaces clinical uncertainty with clear steps for recovery.
What is Actually Causing the Pain?
Ongoing pain after knee replacement is rarely caused by one single issue.
In most cases, the cause sits across three key areas:
The nervous system may already have been sensitised before surgery
Nerves around the knee may have been irritated or injured during surgery
The pain system can remain overactive even after the joint has healed
Understanding which of these is driving your pain is the first step toward effective treatment.
The Hidden Risk Before Surgery
Not all risk starts after surgery.
If you had years of severe discomfort before your operation, understanding how we treat knee arthritis and osteoarthritis helps explain why your pain system may have become sensitised long before the surgery took place.
If you had burning, tingling, or nerve-type pain before your knee replacement, your risk of ongoing pain is higher.
Research shows that pre-existing nerve sensitivity increases the chance of chronic pain after surgery.
This means the nervous system was already sensitised before the operation.
Surgery can fix the joint, but it does not always reset the pain system.
This is one of the most important but often missed factors when assessing ongoing pain after knee replacement.
In this 20-minute masterclass, Dr. Nick Christelis breaks down the "20% Club" and explains how we diagnose the hidden nerve generators that standard X-rays miss.
This video provides general information only and is not a substitute for individual medical advice. Outcomes and treatment suitability vary. Accessing this content does not establish a doctor-patient relationship. Any case studies mentioned are hypothetical.
Some points of interest:
[00:44] Validation: Why pain is real and why it’s not imagined.
[03:45] Plumbing vs. Wiring: Our signature explanation of why the joint (the plumbing) can be perfect while the nerves (the wiring) are faulty.
[05:50] The Saphenous Nerve: Why this specific nerve is the #1 cause of burning pain on the inner side of the knee.
[08:21] The "Night Burn": Why nerve pain peaks when you try to rest and why standard anti-inflammatories fail to stop it.
[09:49] When Light Touch Hurts: Understanding allodynia—why even a bedsheet or clothing can feel like an electrical zap.
[14:10] Diagnostic Blocks: How temporary "numbing tests" can help diagnose sources of pain.
Nerve Sensitivity and Biological Changes
This is the most common reason pain continues after a technically successful knee replacement.
Many people assume that if the surgery was a success, the pain should stop. But the knee contains a complex network of nerves. During knee replacement surgery, small nerves can be irritated, stretched, cut, or trapped in scar tissue.
Identifying specific neural pathways helps find the true cause of chronic post-surgical pain.
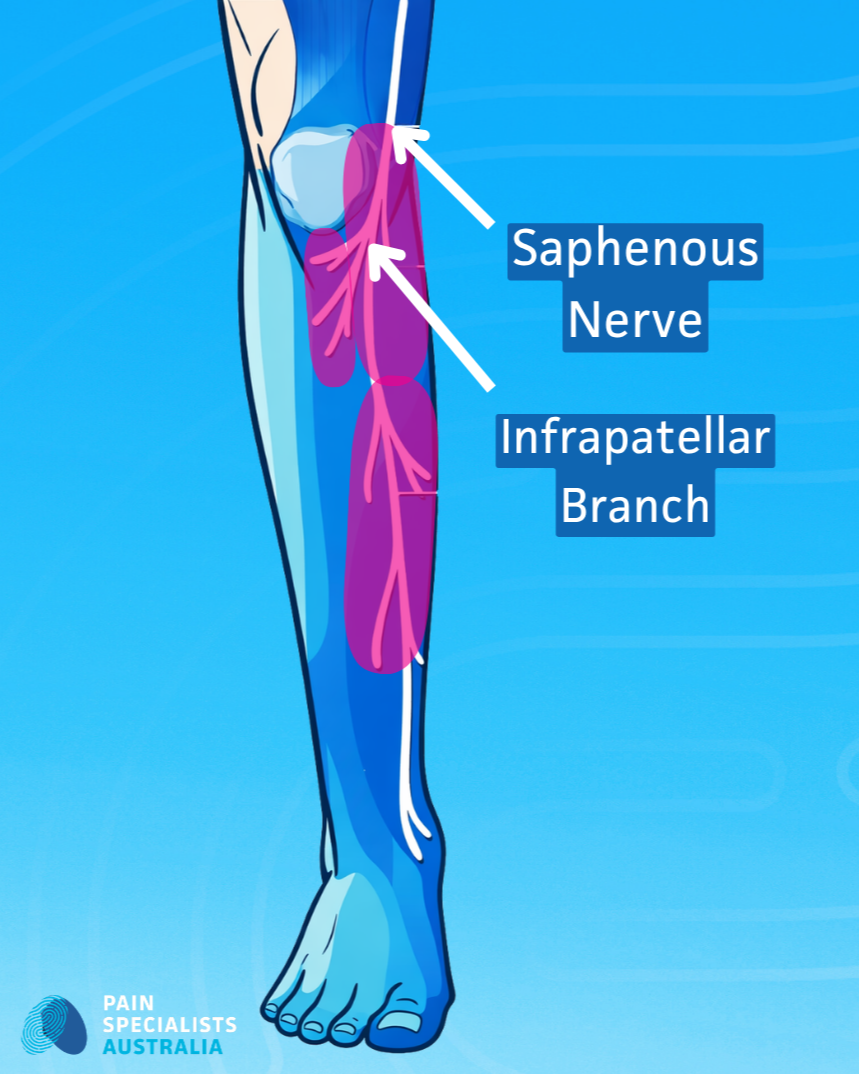
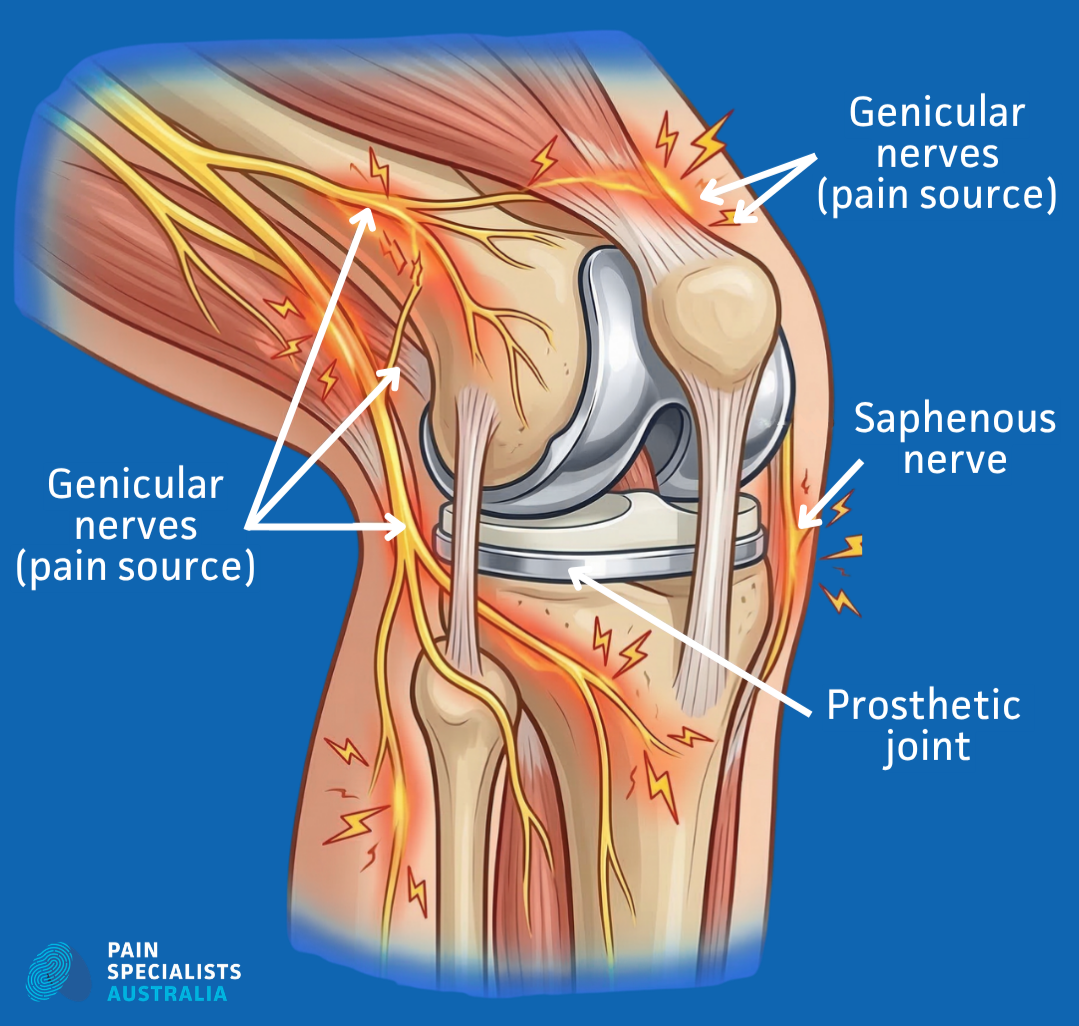
The Saphenous Nerve
A positive Tinel’s sign over the inner knee can help identify this condition.
A common source of medial (inner) knee pain after surgery is the infrapatellar branch of the saphenous nerve. Nerve irritation from surgery or scar tissue causes burning, sharp, or touch-sensitive pain. Such pain does not improve with standard exercise alone.
Involvement of Other Knee Nerves
Other nerves, including branches linked to the common peroneal and obturator nerves, can also contribute to knee pain. When these nerve branches are irritated, pain may be felt on the outer side of the knee or deep within the joint.
Careful diagnosis remains the most important step for recovery.
Identifying the exact nerve branches involved ensures the treatment plan is comprehensive and effective. Targeted diagnostic blocks help confirm which nerves are driving the pain.
Central Sensitisation
When pain lasts for months, the nervous system becomes overactive. The pain system stays switched on, even when the knee is stable.
In simple terms, the entire pain system remains switched on. The process involves peripheral and central sensitisation. Finding the specific nerve responsible is the first step toward a treatment plan.
Could Ongoing Pain Be Complex Regional Pain Syndrome (CRPS)?
Early recognition is critical. Delayed diagnosis can lead to worsening pain and loss of movement.
In some cases, knee replacement surgery can trigger Complex Regional Pain Syndrome, or CRPS. CRPS causes symptoms that go well beyond normal postoperative pain.
People with CRPS often report extreme sensitivity to light touch, changes in skin temperature, and swelling. Early diagnosis is critical to prevent worsening pain, loss of movement, and harder treatment later.
The treatment pathway for CRPS differs from standard surgical recovery.
Targeted Interventional Procedures
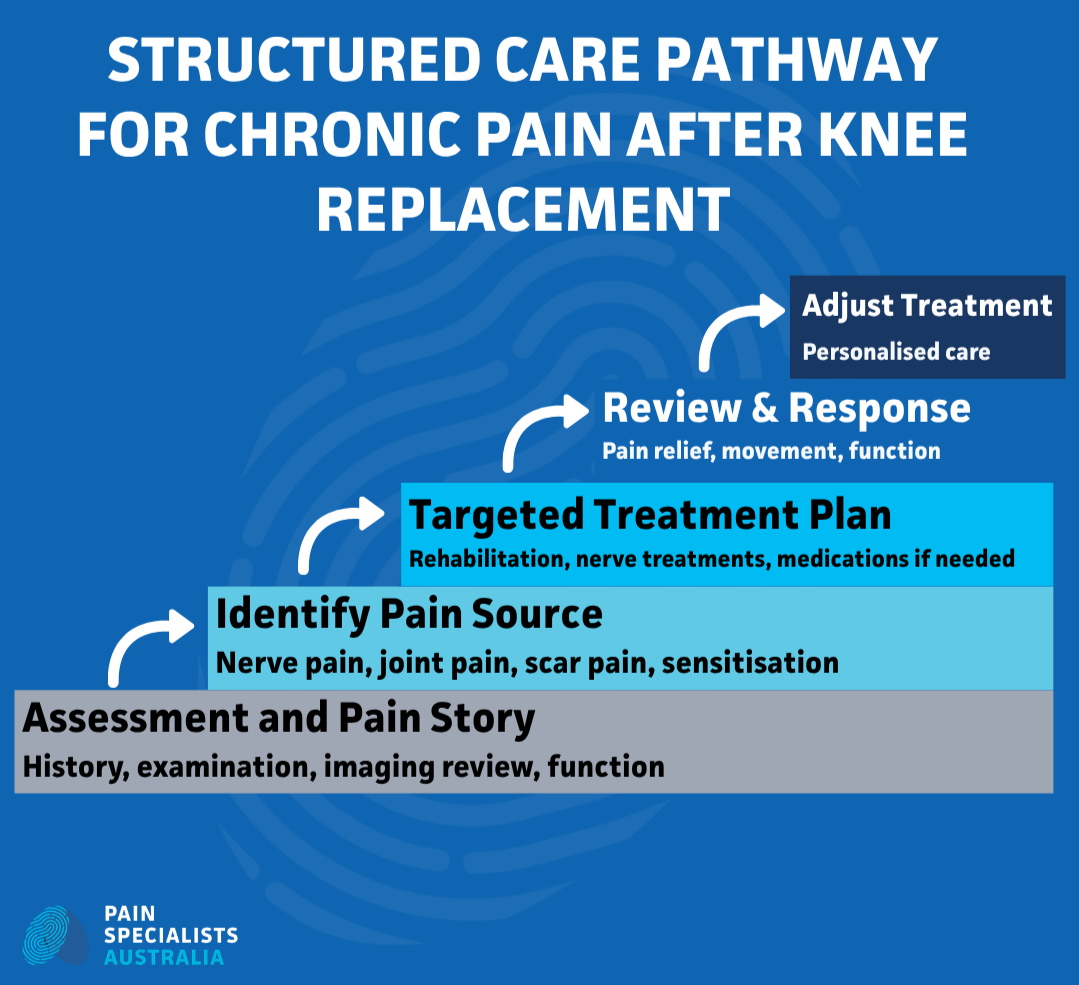
Treatment should follow a clear pathway:
Step 1 – Identify the pain source
Step 2 – Confirm with diagnostic blocks
Step 3 – Apply targeted treatment
Step 4 – Support recovery with rehabilitation
When the diagnosis is clear, targeted procedures help confirm the pain source and reduce the pain signal.
Genicular Nerve Blocks: Diagnostic Precision
A genicular nerve block uses local anaesthetic to temporarily numb the nerves supplying the knee.
If pain improves after the block, the result suggests those nerves are a key part of the pain problem. Diagnostic blocks provide the information needed to guide treatment steps.
While we use diagnostic blocks to find the source of post-op pain, you can also explore how different knee pain injections in Melbourne work to reduce inflammation and support recovery without further surgery.

Precise ultrasound guidance ensures every diagnostic block targets the correct nerve pathway.
Radiofrequency Ablation (RFA): Desensitising the Joint
Radiofrequency ablation uses controlled thermal energy to quieten overactive nerves. Relief often lasts for 6 to 18 months. The window of relief helps patients rebuild strength and progress with rehabilitation.
Neuromodulation for Refractory Nerve Pain
In severe or refractory cases, neuromodulation may help reduce abnormal nerve signalling when other treatments have not been enough.
Why does your knee hurt more at 2 AM? In this episode of The Pain Diaries, Dr. Nick Christelis and Dr. Andy Kwok explores the "Success-Pain Gap." They explore why your nervous system misfires even when surgery is technically perfect. This masterclass is for patients who want to understand the biological "wiring" of their pain.
This video provides general information only and is not a substitute for individual medical advice. Outcomes and treatment suitability vary. Accessing this content does not establish a doctor-patient relationship. Any case studies mentioned are hypothetical.
Fast-track to the answers you need in the video:
[09:16] Plumbing vs. Wiring: Learn why a joint (the plumbing) can be perfect while the nerves (the wiring) are still sending false alarms.
[08:21] The "Night Burn": Why nerve pain peaks when one tries to sleep and why standard painkillers often fail to stop it.
[09:49] When Light Touch Hurts: An explanation of allodynia—why even a bedsheet or clothing can feel like a "zap" or a burn.
[14:28] Beyond the Standard MRI: How a SPECT CT Scan can find the hidden inflammation or bone activity that standard X-rays miss.
[22:52] Specialized Compound Creams: Why we use customized topical treatments (like Ketamine and Clonidine) to quieten sensitized skin nerves.
[32:29] The Spine Connection: Why "knee pain" may be referred pain from the lower back.
[35:12] Radiofrequency Ablation (RFA): How thermal energy can be used to treat pain.
[46:16] The "Nervous System Reset": Can you retrain your brain to stop producing pain after surgery?
Medications to Treat Nerve Pain and Muscle Spasms
Medication management focuses on calming overactive pain nerves, treating nerve pain.
Depending on the pattern of pain, treatment may include medicines used for nerve pain, sleep disruption, or muscle spasm.
One goal is to reduce reliance on opioids where possible.

Managing the pain source creates a window for safe movement and functional recovery.
Restoring Quality of Life: A Holistic Approach
Recovery is about more than pain scores.
Our multidisciplinary approach integrates graded movement, fitness, physiotherapy, sleep support, pacing, and help with flare-ups.
Psychological support can also help with fear, stress, low mood, and the strain of living with ongoing pain
We address every factor to help you restore function and return to daily activities..
Why Choose Pain Specialists Australia?
Your pain is real, even if your scan is normal.
If your pain does not match what your scan shows, it is time to look beyond the joint.
Our doctors are Specialist Pain Medicine Physicians and Fellows of the Faculty of Pain Medicine (FFPMANZCA). Our team has trained in leading centres in Australia and overseas and manages complex pain every day.
Our specialists manage the most complex cases of chronic knee pain in the country, providing a comprehensive clinical pathway for all forms of persistent knee pain, from serious injuries to surgical recovery.
Our focus is simple: make the right diagnosis first, then build the right treatment plan.
We focus on diagnosis first, not trial and error
We use targeted diagnostic blocks to identify the exact pain source
We offer advanced interventional options not widely available
We work with your surgeon and GP
We use a team-based model, with pain specialists and allied health clinicians working together on complex cases.
Once a referral is received, our team aims to contact patients within 24 hours. We arrange assessments at the most convenient Melbourne location, including Richmond, Heidelberg, and Bayside.
Pain Specialists Australia is one of the largest private pain clinics in Australia, with a strong focus on advanced diagnosis and interventional pain care.
Learn more about our full clinical pathway for all forms of knee pain.

Frequently Asked Questions (FAQ)
1. Why does my knee still hurt if the surgeon says the X-ray is perfect?
X-rays show the implant and joint alignment, but they do not show how the surrounding nerves are functioning (Banks et al. 2025). Chronic discomfort often results from nerve irritation and biological sensitisation rather than mechanical failure. A normal scan confirms the joint is stable while signalling the need to investigate neural pain generators.
2. Is nighttime burning pain common six months after a knee replacement?
Burning pain at night can be a sign of nerve irritation or pain sensitisation after knee replacement (Wylde 2011). Nerve branches like the infrapatellar saphenous nerve become hyper-sensitive and fire spontaneous pain signals during rest. Recognising the symptoms allows specialists to move from general rehabilitation to targeted nerve treatments.
3. Could the pain be Complex Regional Pain Syndrome (CRPS)?
Complex Regional Pain Syndrome is a pain condition that can sometimes be triggered by surgery.
The nervous system produces an exaggerated inflammatory response involving temperature changes, swelling, and extreme touch sensitivity. Early clinical identification is vital to prevent long-term functional loss (Gooberman-Hill 2023).
4. How do you help patients reduce reliance on opioids?
Nerve-driven pain typically responds poorly to traditional opioid medications and requires a broader management strategy (ACSQHC 2024). Opioids often do not work well for nerve-driven pain because they do not target the real pain mechanism.
Targeted interventions and non-opioid medications provide better functional recovery with fewer systemic side effects.
5. What is a genicular nerve block?
A genicular nerve block is a diagnostic procedure used to pinpoint the exact source of joint pain (Bogduk 2002). If numbing the knee nerves reduces the pain, it suggests those nerves are an important pain source.
Successful temporary relief provides the clinical evidence needed to proceed with long-term treatments.
6. Can I still do physio if my knee is sensitised?
The right exercises, done at the right stage and pace, can help calm the pain system and improve movement.
Specific exercises in combination with pain neuroscience education can reduce neural sensitisation (Larsen 2025). Coordinating therapy with pain-relieving procedures creates a safe window for restoring movement.
7. How long does relief from radiofrequency ablation (RFA) last?
Radiofrequency ablation often provides pain relief for several months, and sometimes much longer (Caragea 2023). The thermal energy stuns overactive nerves, interrupting the transmission of pain signals to the brain. The extended period of relief allows patients to engage in rehabilitation and reclaim daily activities.
8. Why is early diagnosis so important?
Early diagnosis prevents the transition from acute post-surgical soreness to chronic central sensitisation.
Early diagnosis helps stop ongoing pain from becoming more entrenched and harder to treat (Gonzalez 2025). Prompt interventional care settles the nervous system before neural changes become harder to reverse.
9. How do you know if pain is coming from a nerve after knee replacement?
Nerve pain often feels burning, sharp, or sensitive to touch.
The most reliable way to confirm this is with targeted diagnostic blocks.
If numbing a specific nerve reduces the pain, it confirms the source.
References
Research helps guide how chronic pain after knee replacement is diagnosed and treated.
1. Banks DW, Park H, Oehlermarx W, et al. Chronic Post-Surgical Pain After Hip and Knee Arthroplasty: An Update on Mechanisms, Risk Factors, and Interventional Treatment Modalities. J Pain Res. 2025;18:6205-6219. Published 2025 Nov 20. doi:10.2147/JPR.S546617
The review highlights the transition from structural healing to chronic nerve sensitisation.
https://pubmed.ncbi.nlm.nih.gov/41293079/
2. Wylde V, Hewlett S, Learmonth ID, Dieppe P. Persistent pain after joint replacement: prevalence, sensory qualities, and postoperative determinants. Pain. 2011;152(3):566-572. doi:10.1016/j.pain.2010.11.023
Research confirms that approximately 15% of patients experience ongoing distress after surgery.
https://pubmed.ncbi.nlm.nih.gov/21239114/
3. Gooberman-Hill R, Wylde V, Bertram W, et al. Better post-operative prediction and management of chronic pain in adults after total knee replacement: the multidisciplinary STAR research programme including RCT. Programme Grants for Applied Research. 2023;11(3). Bethesda (MD): National Center for Biotechnology Information (US). doi:10.3310/WATM4500
The large-scale study identifies risk factors and develops pathways for managing long-term post-operative pain.
https://www.ncbi.nlm.nih.gov/books/NBK593420/
4. Caragea M, Woodworth T, Curtis T, et al. Genicular nerve radiofrequency ablation for the treatment of chronic knee joint pain: a real-world cohort study with evaluation of prognostic factors. Pain Med. 2023;24(12):1332-1340. doi:10.1093/pm/pnad095
The clinical data demonstrates the efficacy of thermal treatment in reducing chronic joint pain for up to two years.
https://pubmed.ncbi.nlm.nih.gov/37428157/
5. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745-1759. doi:10.1016/S0140-6736(19)30417-9
Clinical guidelines advocate for a transition from structural imaging to functional and biological care.
https://pubmed.ncbi.nlm.nih.gov/31034380/
6. Giannetti A, Valentino L, Giovanni Mazzoleni M, Tarantino A, Calvisi V. Painful total knee arthroplasty: Infrapatellar branch of the saphenous nerve selective denervation. A case series. Knee. 2022;39:197-202. doi:10.1016/j.knee.2022.09.010
High-resolution imaging confirms the involvement of the saphenous nerve in persistent medial knee pain.
https://pubmed.ncbi.nlm.nih.gov/36209652/
7. Bogduk N. Diagnostic nerve blocks in chronic pain. Best Pract Res Clin Anaesthesiol. 2002;16(4):565-578. doi:10.1053/bean.2002.0252
This explains how diagnostic blocks can be used to diagnose pain sources.
https://pubmed.ncbi.nlm.nih.gov/12516892/
8. Gonzalez FF, Barone A, Palaniappan R, et al. Preoperative neuropathic-like pain and central sensitisation are risk factors for chronic pain after total knee arthroplasty: A systematic review and meta-analysis. Osteoarthr Cartil Open. 2025;7(4):100674. Published 2025 Aug 29. doi:10.1016/j.ocarto.2025.100674
The article explains how preoperative screening identifies preexisting nerve sensitisation as a risk factor.
https://pmc.ncbi.nlm.nih.gov/articles/PMC12454881/
9. Australian Commission on Safety and Quality in Health Care. (2024). Osteoarthritis of the Knee Clinical Care Standard. Sydney: ACSQHC.
The national standard prioritises evidence-based care pathways and reduced reliance on ineffective interventions.
10. Larsen JB, Skou ST, Laursen M, Bruun NH, Madeleine P, Arendt-Nielsen L. Pain Mechanisms and Psychosocial Variables in Patients With Chronic Pain After Total Knee Arthroplasty: Secondary Analysis From a Randomised Controlled Trial. Eur J Pain. 2025;29(6):e70064. doi:10.1002/ejp.70064
The study confirms that exercises combined with pain neuroscience education reduce sensitisation.
